




Welcome to the Best FREE National Academy of Sports Medicine (NASM) Certified Personal Trainer Study Guide in 2026.
We promise all the tools to help you become a successful NASM Certified Personal Trainer.
Be sure to Bookmark!
This page is crafted for the layout of the NASM 7th Edition text; if you would like the 6th Edition layout, check it out here.
Let’s get to it!!
Domain 1: Professional Development and Responsibility
Don’t forget to download our 14 step NASM CPT exam preparation checklist to ensure that you pass the test.
Check out our premium NASM CPT MVP study materials here. Reduce your study time by half and receive an exam pass guarantee.
Section 1. Professional Guidelines and Standards
1. Do not diagnose or treat illness or injury unless for basic first aid or if the Certified Professional is legally licensed to do so and is working in that capacity at that time.
2. Do not train clients with a diagnosed health condition unless the Certified Professional has been specifically trained to do so.
3. Do not begin to train a client prior to receiving and reviewing a current health-history questionnaire signed by the client.
4. Hold a current cardiopulmonary resuscitation (CPR) and automated external defibrillator (AED) certification from a NASM-approved provider at all times.
Section 2. Business Fundamentals
Making informed predictions based on previous performance indicators and existing trends.
- Decide on an income figure
- Identify weekly earnings required for that goal
- Calculate the number of required weekly sessions
- Identify the required closing percentage
- Create a client conversion timeline
- Identify the total number of interactions required based on the closing percentage
- Identify the required amount of daily interactions
- Do an hour-by-hour daily breakdown of interactions
- Make sure you obtain contact information
- Conduct follow-ups
Section 3. Marketing Concepts and Techniques
1 – Product
2 – Price
3. -Placement
4 – Promotion
Section 4. Sales Concepts and Techniques
Implementation of methods designed to search for new clients.
- Empathize with and understand the client’s concerns
- – Isolate the actual drawbacks
- – Remind the client of the benefits
- – Make a plan to resolve concerns
Domain 2: Client Relations and Behavioral Coaching
Section 1. Communication Components
- Use of appropriate body language
- Explain important concepts
- Show empathy and compassion
- Use positive reinforcement
- Use positive greeting protocols (smile, handshake. hello)
Visual and auditory expressions of intent and feeling that exist outside of written or spoken speech.
Practicing listening as an act of genuine interest.
Open-ended questions allow the questioned party to elaborate with detail. Close-ended questions only require a yes or no answer.
Relaying back your interpretation of what the client has communicated.
Making brief reflections on what has been communicated to indicate that information has been taken on board.
Section 2. SMART Goals
S- Specific
M- Measurable
A- Attainable
R- Realistic
T- Timely
Section 3. Goal Expectation Management
1. Understand the client’s motivations
2. Hone in and clarify vague statements like “I want to get fit” or “I want to look better.”
3. Allow clients to verbalize their goals for more clarity
4. Identify unrealistic outcomes
5. Set goals based on the SMART principles
6. Be able to contrast between product and progress-based goals
7. Be aware that progress occurs at different rates for different clients
8. Identify how and when each client’s goals will be reassessed and revisited
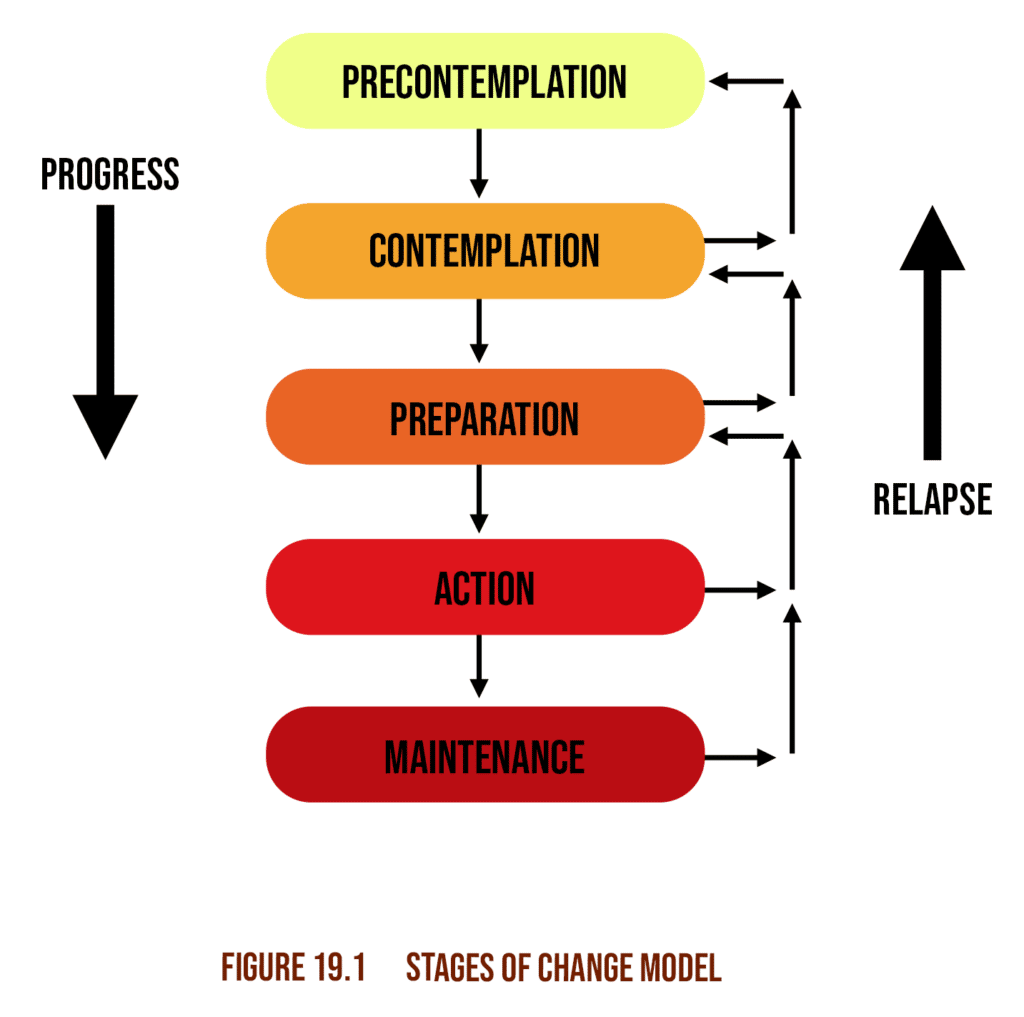
Section 4. Behavior Change Strategies
Try to think of the stages without seeing the chart below, first.
– Instrumental support in the form of practical applications and infrastructure
– Emotional support in the form of positive psychological reinforcement and encouragement
– Informational support in the form of facts and evidence that provide direction and indicate efficacy and reliability
– Companionship support in the form of positive social associations such as family and close friends
Section 5. Psychological Response to Exercise
– Promotes positive mood
– Improves the quality and quantity of sleep
– Reduces stress
– Reduces indicators and risk factors of anxiety and depression
Section 6. Barriers to Behavior Change
- Time constraints
- Setting unrealistic goals
- Inadequate social support
- Social anxiety and low self-esteem, Convenience or addictiveness of current behavioral patterns
Section 7. Client Expectation Management
- If the client is ready to begin or has any further questions/queries
- – The social dynamics, etiquette, and training culture of the facility
- – Dress code
- – The potential outcomes of interactions with other clients/members
Domain 3: Basic and Applied Sciences and Nutritional Concepts
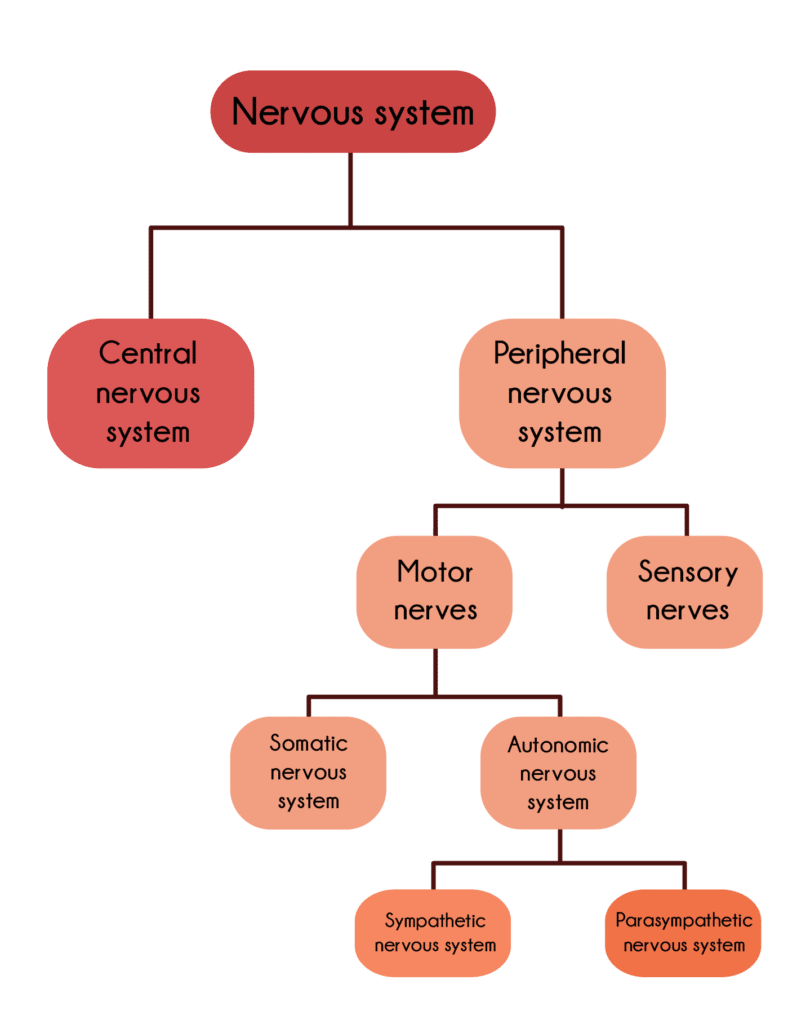
Section 1. The Nervous System
Golgi Tendon Organ – GTOs are specialized sensory receptors located at the point where skeletal muscle fibers insert into the tendons of skeletal muscle.
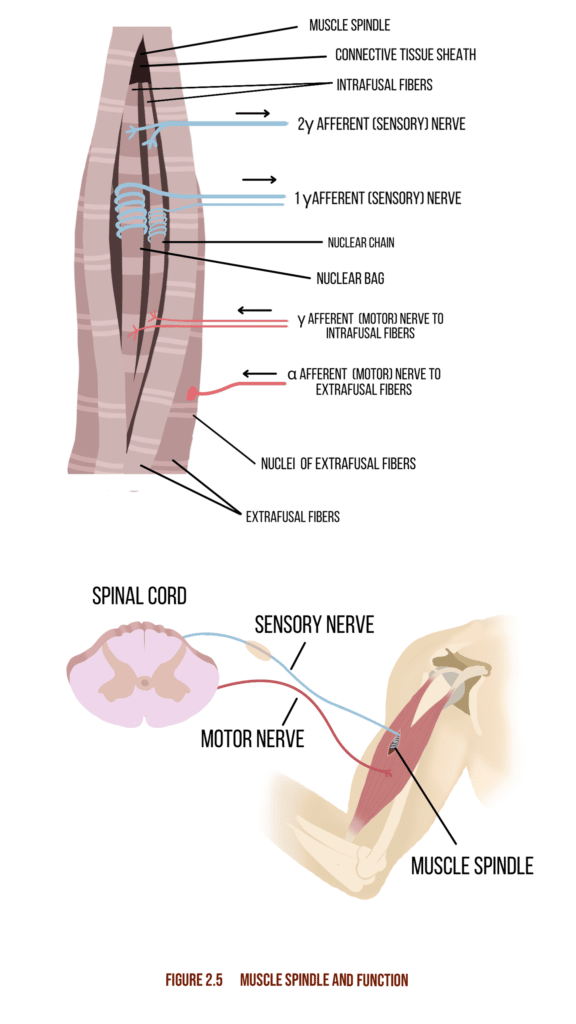
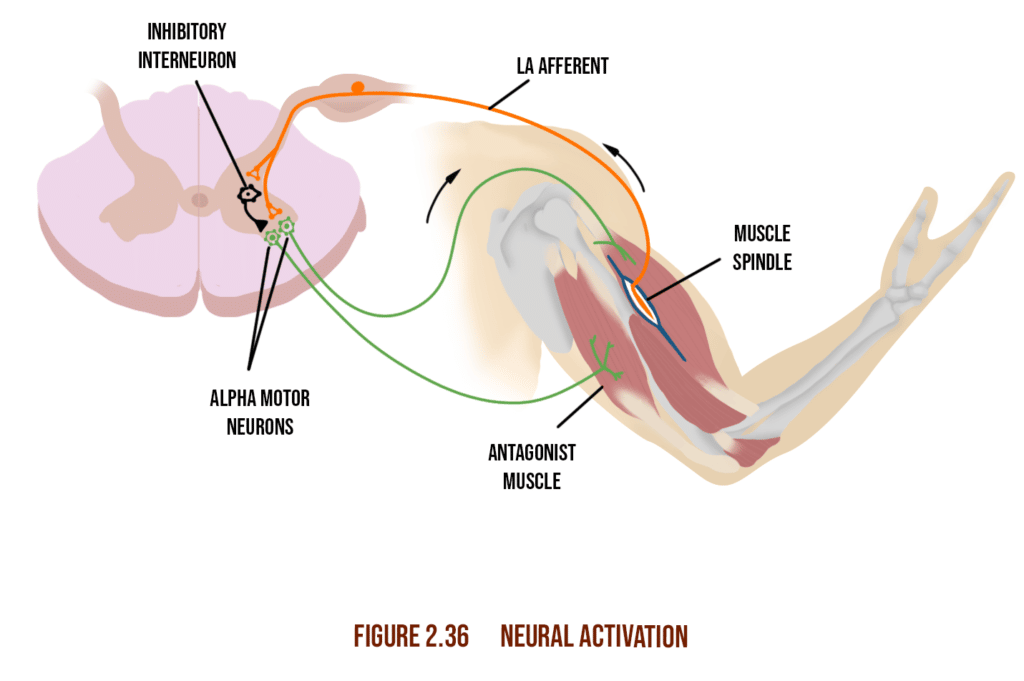
Muscle Spindle – Muscle Spindles are sensory receptors within muscles that run parallel to the muscle fibers and are sensitive to changes in muscle length and rate of length change.
The Charts below are found in chapter 5 of the 7th edition.
These figures are found in lesson 1 of chapter 5 in the 7th edition text.
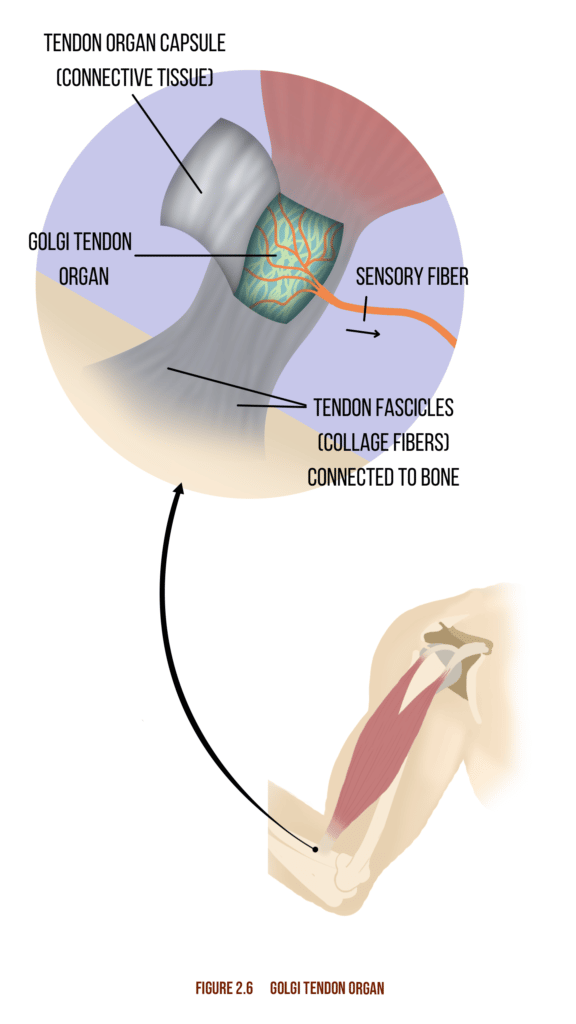
The three primary functions of the nervous system include sensory, integrative, and motor functions. Sensory Function is the ability of the nervous system to sense changes in either the internal or external environment. Integrative Function is the ability of the CNS to analyze and interpret sensory information to allow for proper decision-making, which produces an appropriate response. Motor Function is then the body’s response (via the efferent pathway) to that integrated sensory information, such as causing a muscle to contract when stretched too far or changing one’s walking pattern when transitioning from walking on a sidewalk to walking in the sand.
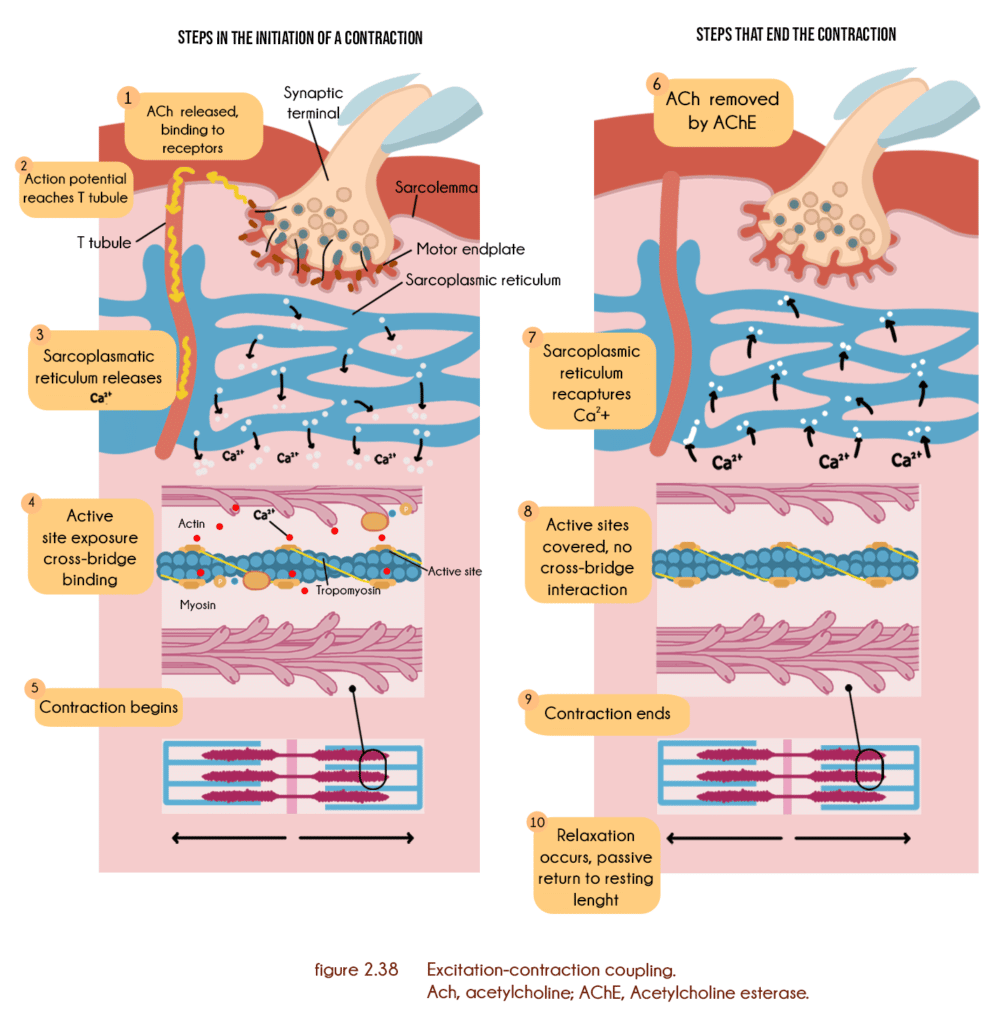
These figures can be found throughout lesson 1 of chapter 5 in the 7th edition text.
Section 2. The Muscular System
Tendons- Connective tissue bridging muscles to the skeleton
Fascia- Connective tissue that consists of a tough fibrous membrane that holds muscle tissue together
Fascicles- Muscle fiber units bundled within a single muscle
Muscle fiber- Cylindrical cells that produce and resist force through mechanical contraction, allowing organisms to move and reposition
Sarcomere- The muscle fiber’s fundamental contractile unit consisting of protein filaments actin and myosin
Sliding filament theory- That contraction of muscles takes place through the sliding of actin and myosin
Type I (slow-twitch) muscle tissue- Predominantly aerobic muscle fibers responsible for sustained, focused contractions and have a relatively higher mitochondrial count for that reason
Type II (fast-twitch) muscle tissue- More anaerobic, these fibers are tasked with short, explosive contractions aimed at generating power and speed
Motor unit- The smallest functional unit of a muscle and motor unit system
Neural activation- The stimulation of motor units through the delivery of mild impulses. Also known as warming up.
Neurotransmitters- A signaling chemical release at the end of nerve synapses used to transfer impulses across nerve junctions or to muscle fibers
The chart is found in lesson 4 of chapter 5 in the 7th edition.

Local stabilization system- Muscle system connected directly to vertebrae
Global stabilization system- Muscle system that transfers force between the upper and lower body, thus providing full-body stability
Movement system- All organs and structures whose collective function brings about mobility and biomechanical activity. These figures are found throughout lesson 4 of chapter 5 in the 7th edition text.
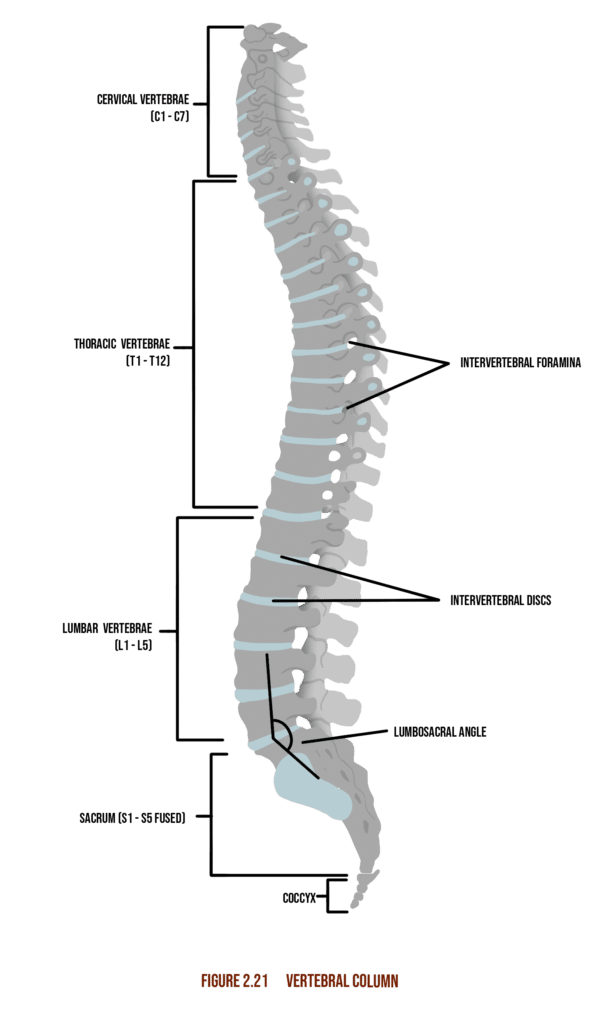
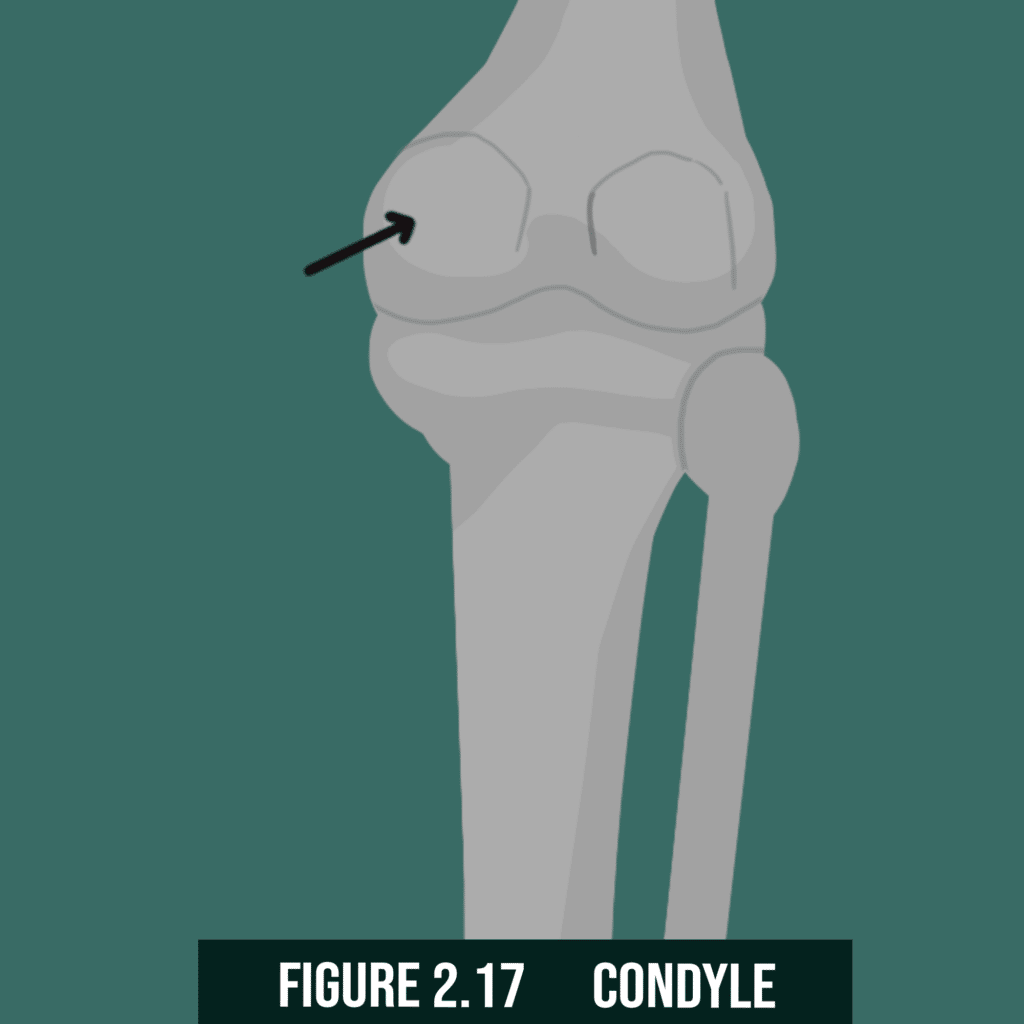
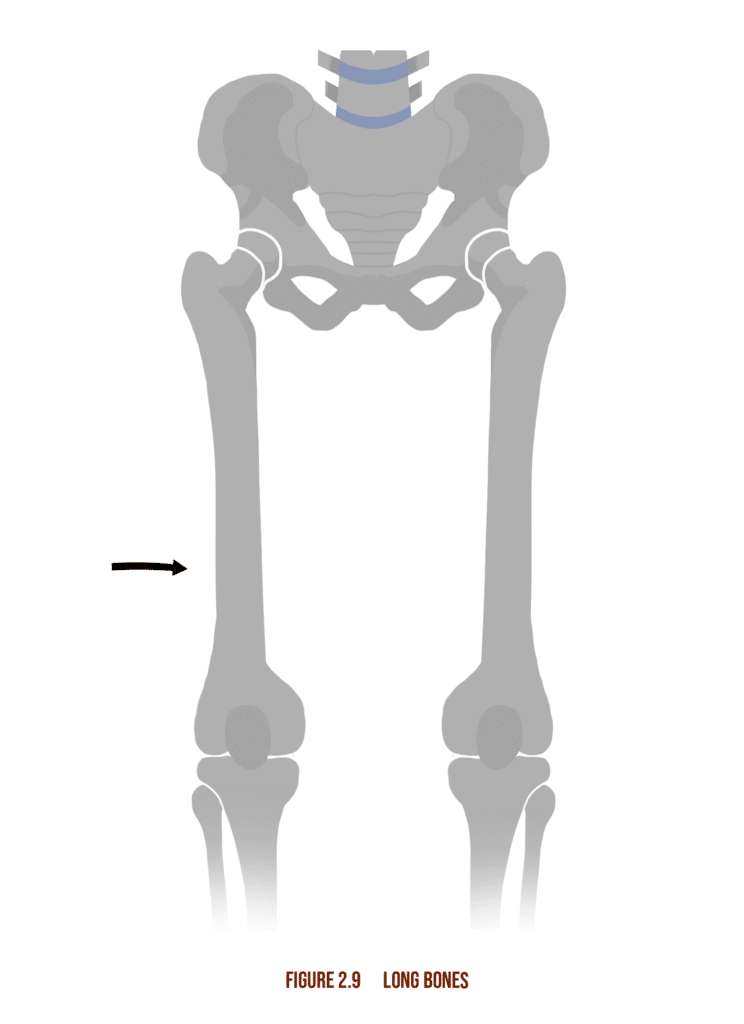
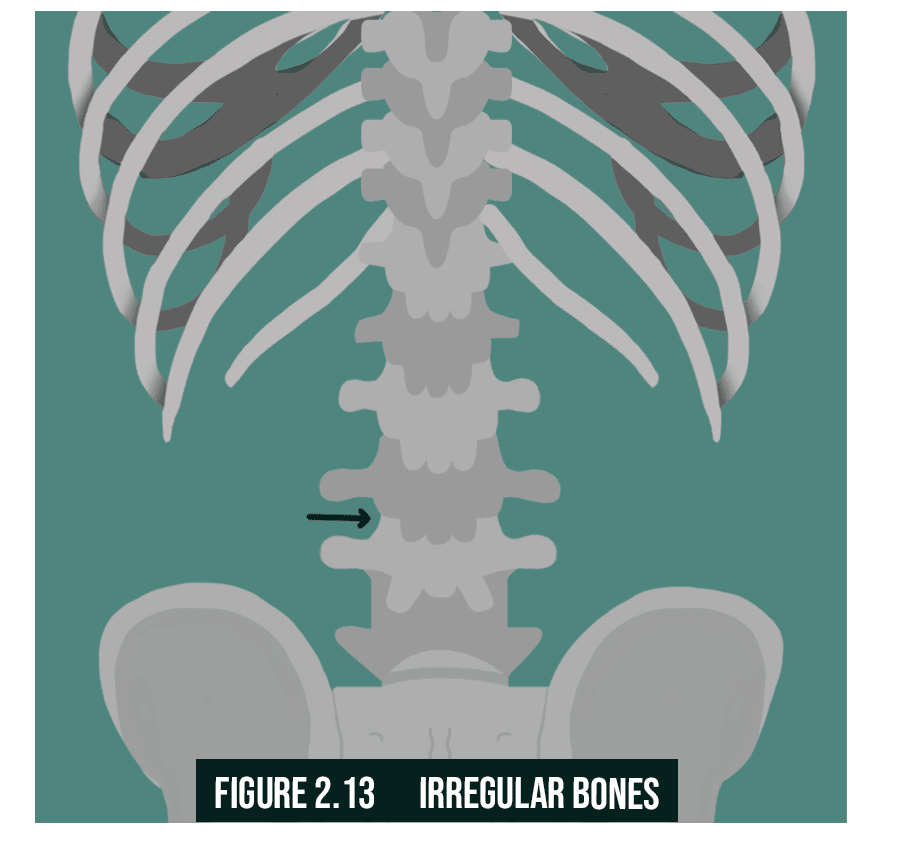
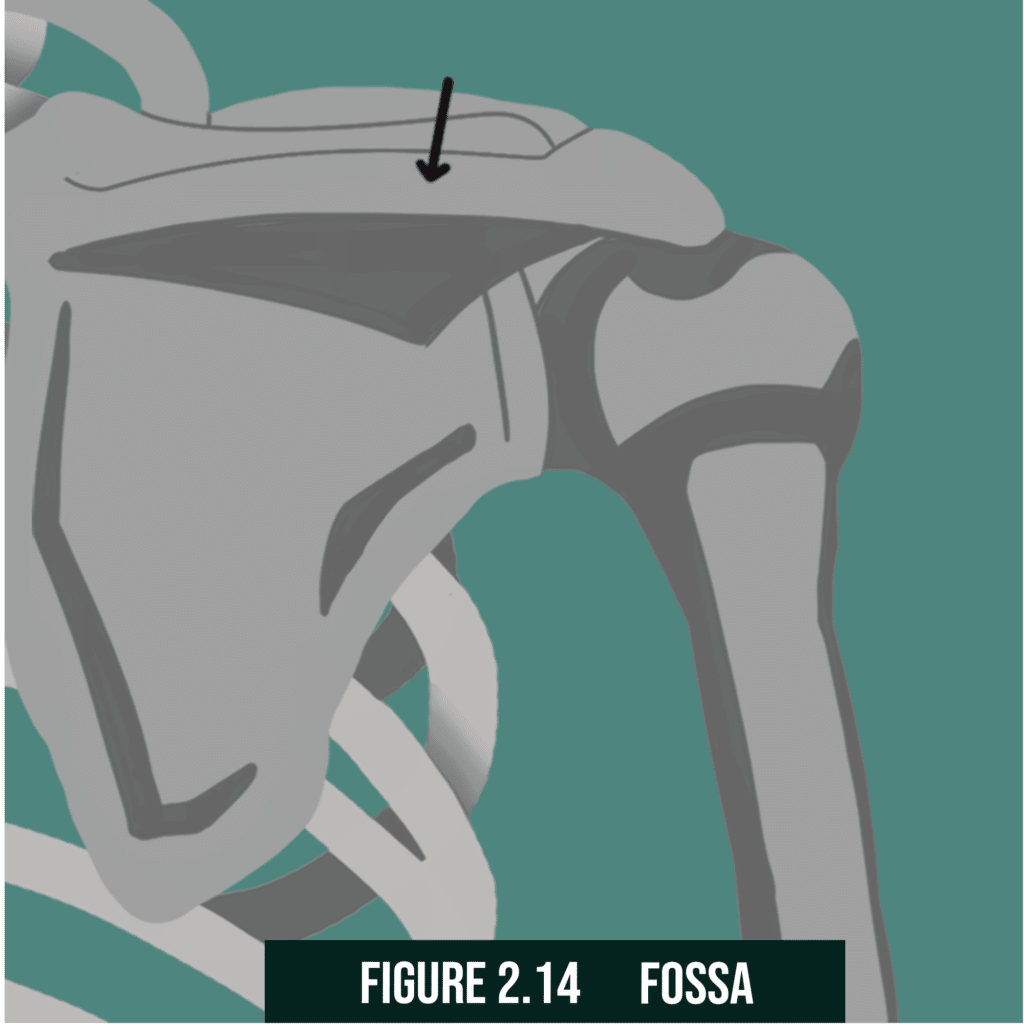
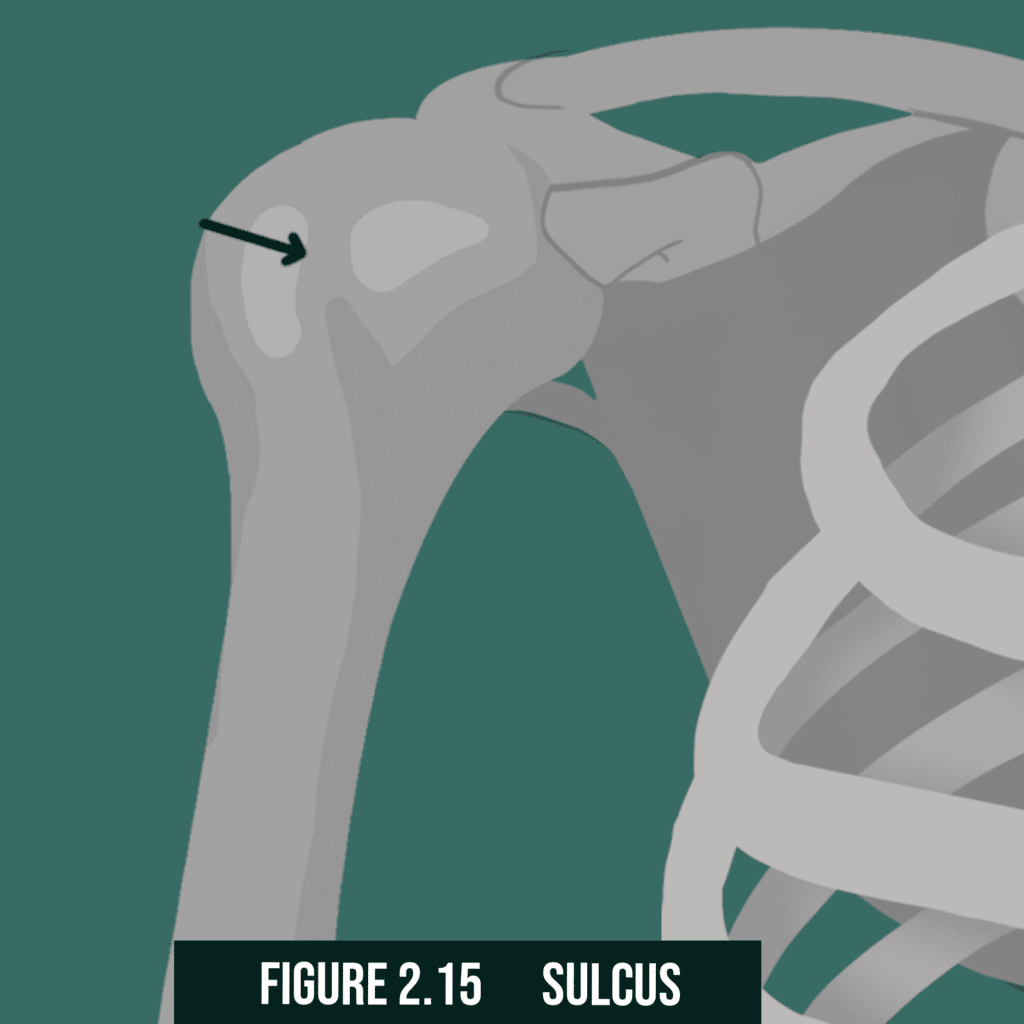
Section 3. The Skeletal System
These diagrams are found throughout chapter 5, lesson 2.
Joints are the sites where two bones meet, and movement occurs as a result of muscle contraction.
These images are found throughout lesson 2 of chapter 5 in the 7th edition.
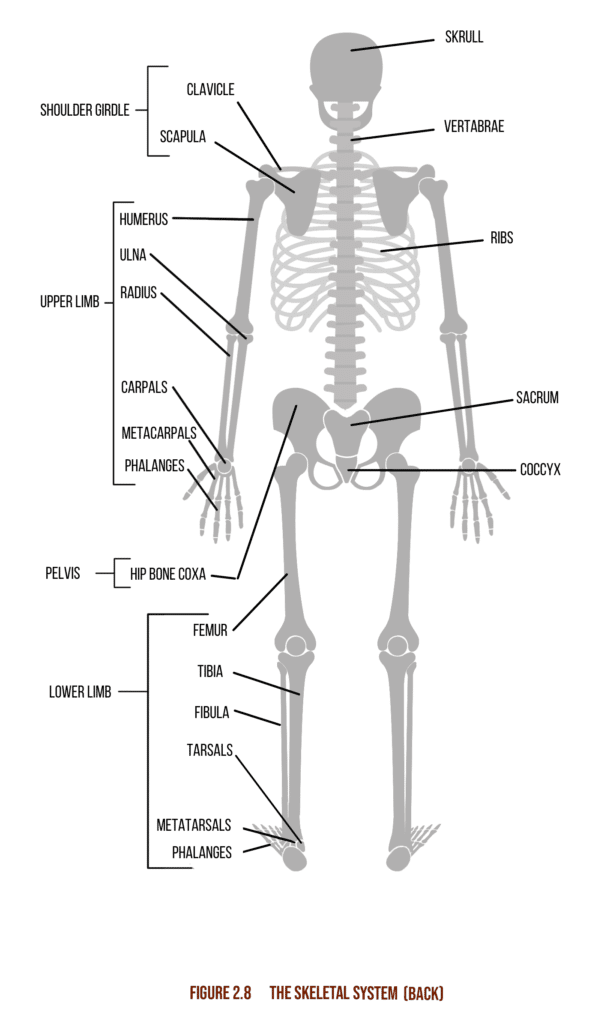
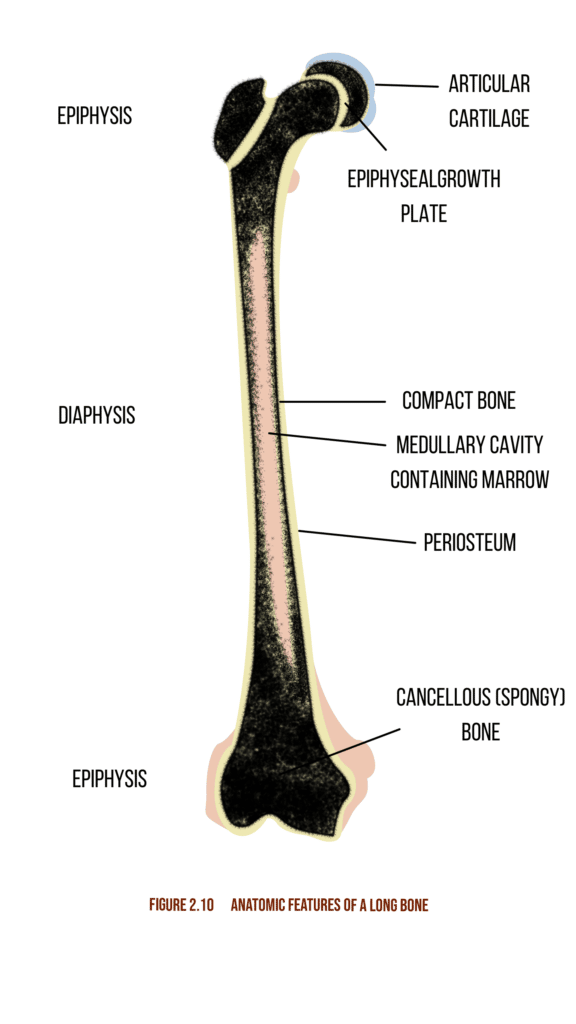

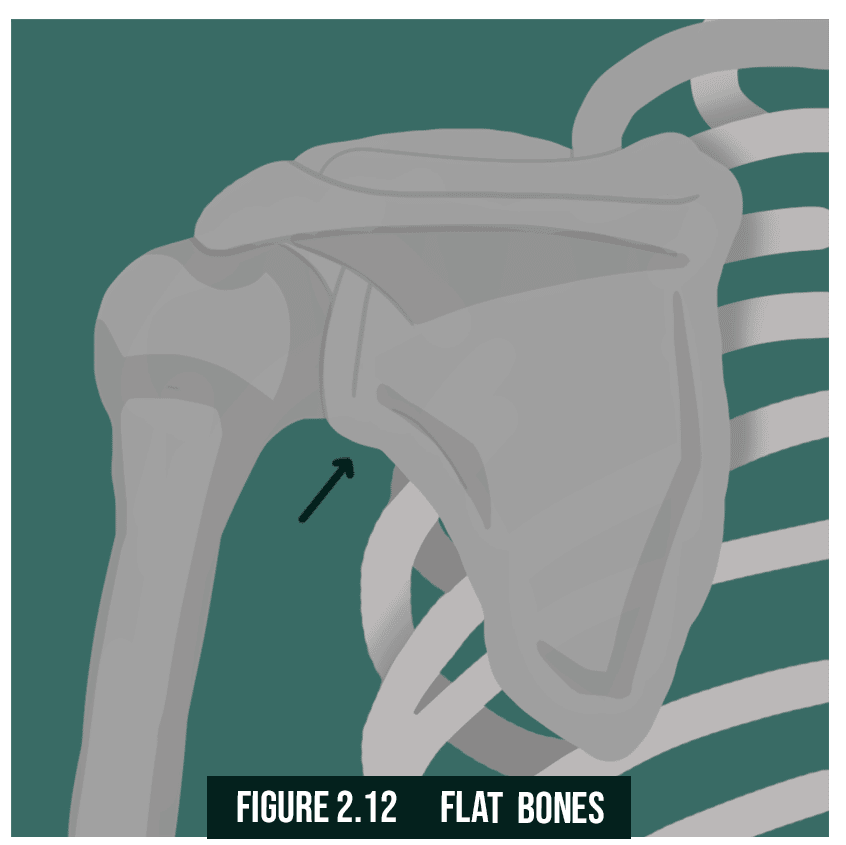
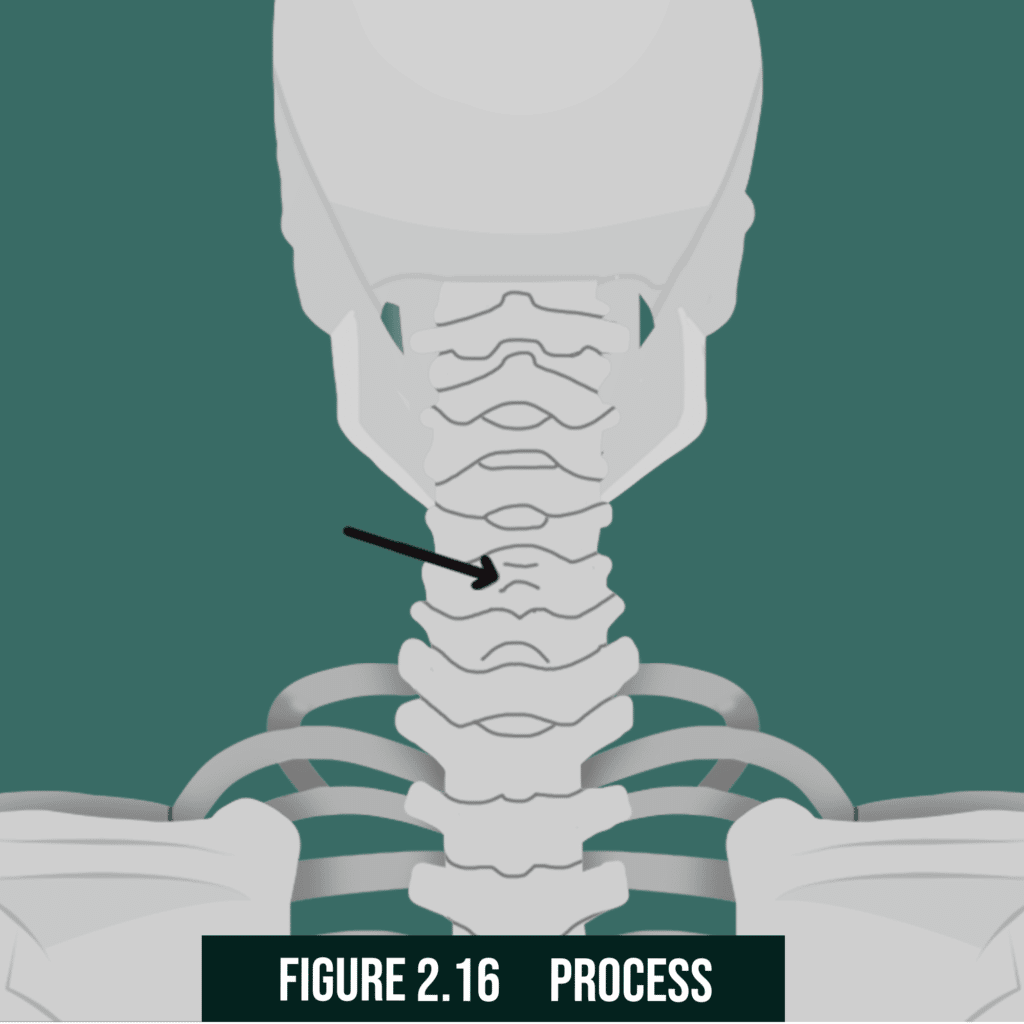
Skeletal system functions- Structural integrity and support, protection of vital organs, mobility, anchoring of organs, production of blood and endocrine hormones
Non-synovial joints- Maintains structural integrity by joining bone segments not required to perform a movement
Synovial Joints- Joints that allow smooth movement between two or more adjacent bones
Major motion types- Spin, slide, and roll
Hinge Joint- Sagittal plane. E.g. elbows and knees
Ball-and-socket Joint- Full axis mobility. E.g. Pelvic and shoulder girdle
Arthrokinematics- The science of joint motion
Section 4. The Endocrine System
Endocrine system- The system responsible for the production and secretion of hormones
Testosterone- Anabolic male sex hormone
Estrogen- Female sex hormone
Growth hormone- Anabolic tissue growth hormone
Insulin- Energy and micronutrient regulation hormone
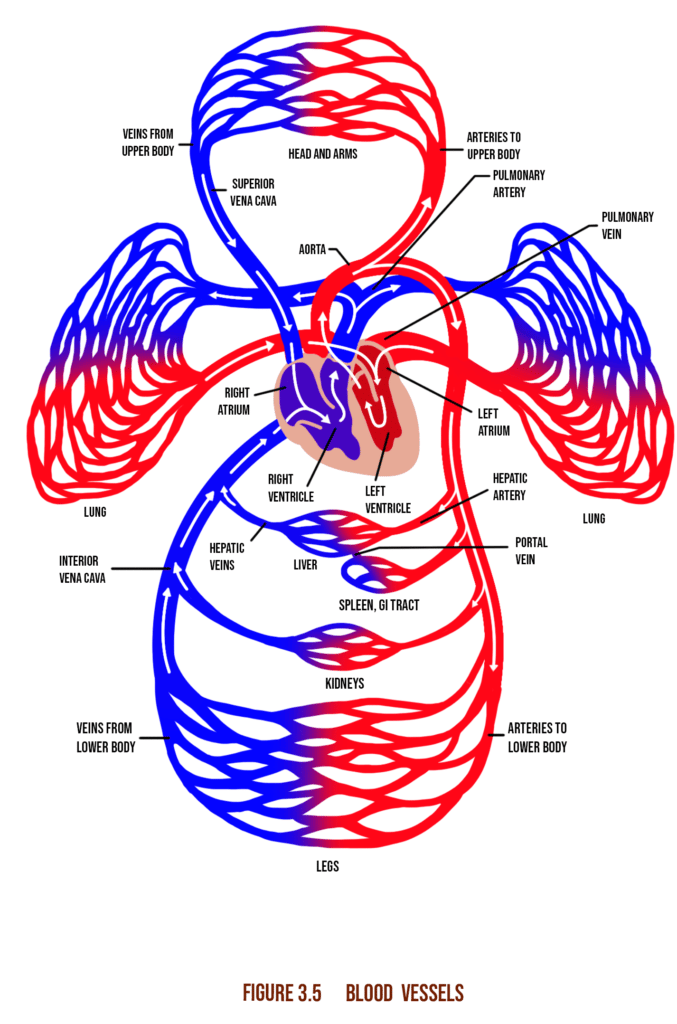
Section 5. The Cardio-respiratory System
Cardiorespiratory system- System comprised of the heart, blood vessels (circulatory), and lungs (respiratory)
Cardiovascular system- The heart and blood vessels
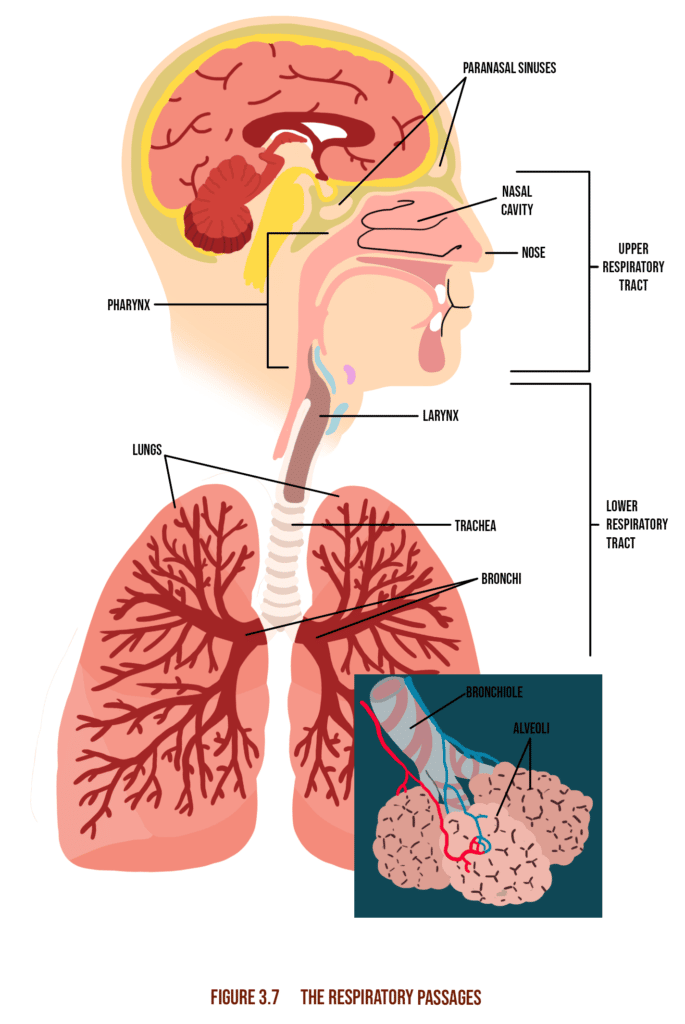
Respiratory system- Lungs and breathing system
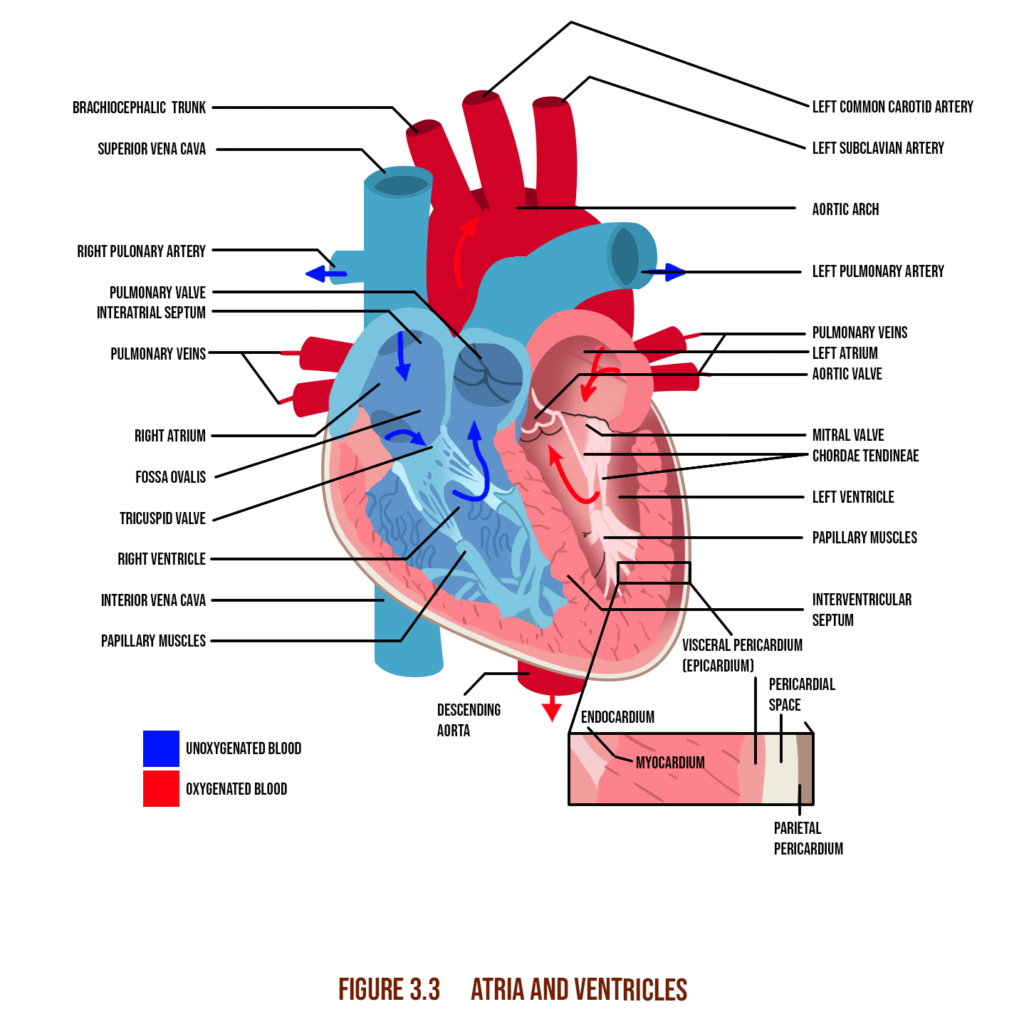
Cardiac muscle- Involuntary heart muscle, relatively more rigid than skeletal muscle
Right atrium- Gathers low-oxygen blood
Left atrium- Gathers oxygenated blood from the lungs
Sinoatrial (SA) node- Myocyte clusters that generate electrical impulses that determine heart rhythm
Right ventricle- Pumps low oxygen blood to lungs
Left ventricle- Pumps oxygen-rich blood through the body
Arteries- Vessels for oxygenated blood
Veins- Vessels for deoxygenated blood
Arterioles- Small branches of arteries
Capillaries- Smallest blood vessel units. Chemical exchange sites
Venules- Smallest branches of veins
Stroke volume- The volume of blood circulated with each pump
Heart rate- The frequency of heartbeats per minute
Cardiac output- Amount of blood pumped per minute
Inspiration- Moving air into the lungs through muscular contractions
Primary inspiratory muscles- External intercostals and diaphragm
Secondary inspiratory muscles- scalenes, sternocleidomastoid, and pectoralis minor
Expiration- Pushing air out of the lungs through muscular contraction
Expiratory muscles- Abdominals and internal intercostals
Resting oxygen consumption (VO2)- Amounts to 3.5ml/min/kg of body mass and is the equivalent of 1 metabolic equivalent (MET)
Maximal oxygen consumption (VO2max)- Maximum oxygen consumption rate at peak exercise intensity
Dysfunctional breathing- Irregular breathing patterns characteristic of stress and anxiety
Increases: metabolic activity, mental alertness, cardiac function, respiratory function.
Decreases: resting heart rate, LDL cholesterol, blood pressure, risk of cardiovascular disease.
These diagrams are found throughout lesson 1 of chapter 6 in the 7th edition text.
Transport- Oxygen, nutrients, and hormones
Regulation- Temperature, fluid balance, pH
Protection- Immune system, clotting
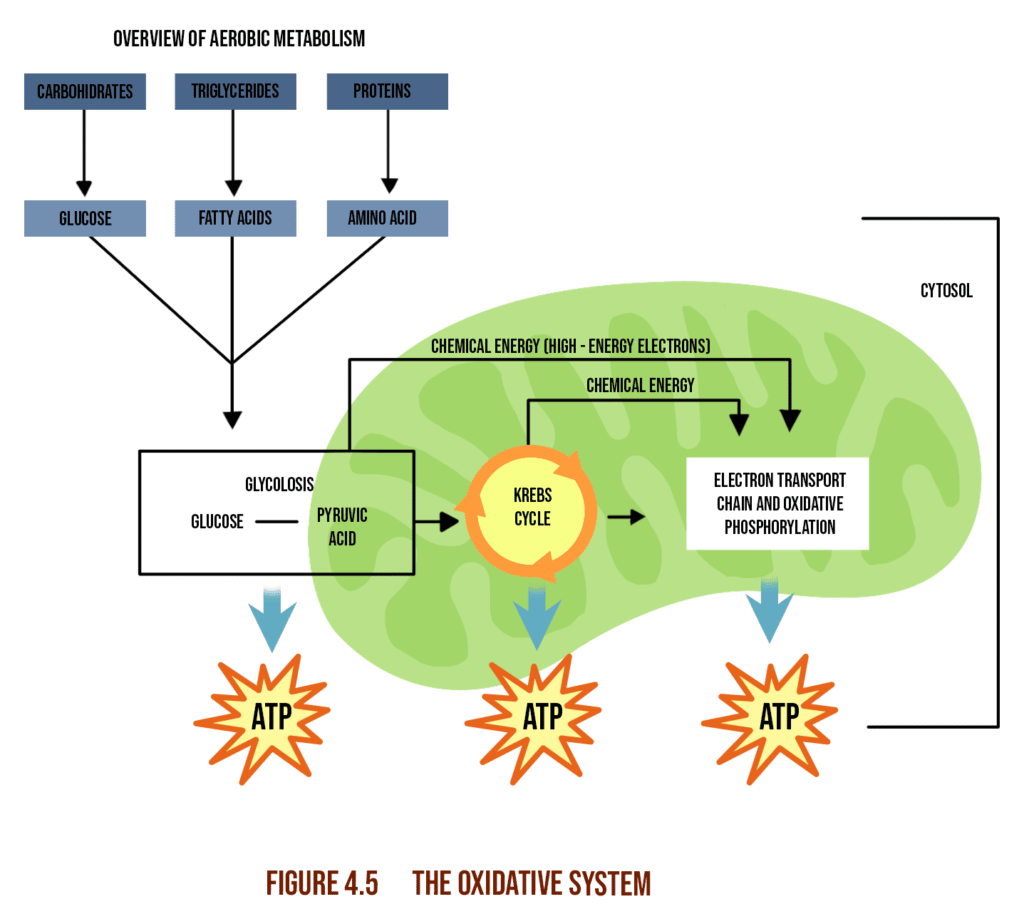
Section 6. Bioenergetics and Exercise Metabolism
Bioenergetics- The science of energy in the body
Metabolism- The usage cycle of nutrients and their conversion into energy, body components, and waste materials through normal life function
Aerobic- Using oxygen to drive metabolic function
Anaerobic- Metabolic activity with an absence of oxygen
Adenosine triphosphate (ATP)- A molecule used to transfer and store energy in cells
Anaerobic threshold- The point at which energy demand surpasses oxygen supply
Excess postexercise oxygen consumption(EPOC)- Post-exercise elevated metabolic activity
Oxidative- Aerobic glycolysis, Krebs cycle, electron transport chain, Long-term energy
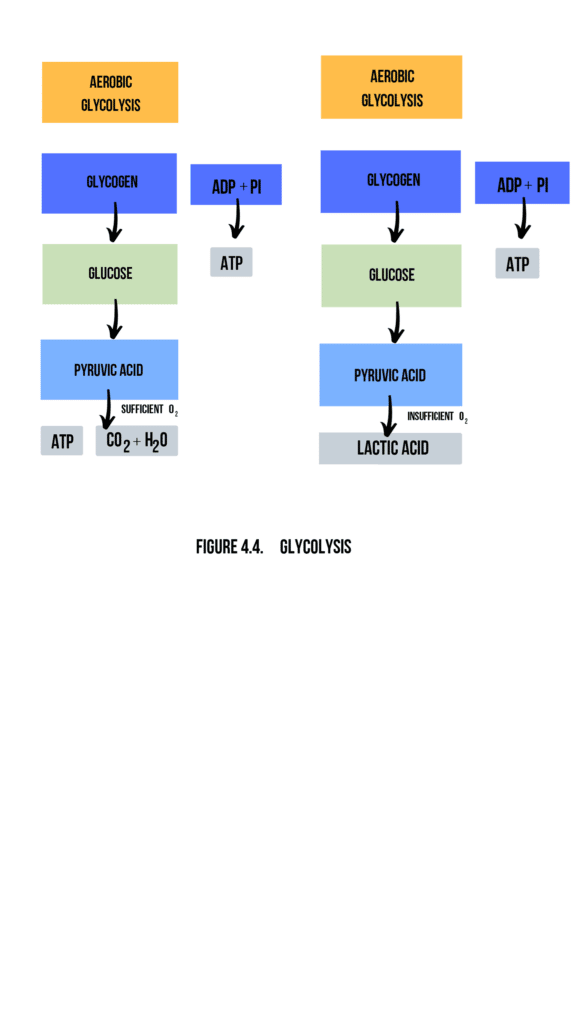
Glycolysis- Anaerobic, Moderate-to-high intensity, lasts up to 30-50 seconds
ATP-PC- Anaerobic, High-intensity, Lasts up to 10-15 seconds
Section 7. Fundamentals of Biomechanics
The science concerning the generation, transfer, and resistance of mechanical force by the musculoskeletal system and the effects produced.
A transfer of energy that acts on a physical body causing it to change its direction and velocity.
A rotational force acting about a fixed axis.
A rigid bar that applies torque about a fixed pivot or fulcrum.
1st class- The fulcrum in the center
2nd class- Resistance in the center
3rd class- Effort in the center
Section 8. Anatomic locations
Superior- Above
Inferior- Below
Proximal- Closest to a reference point
Distal- Furthest from a reference point
Anterior- front
Posterior- behind
Medial- central
Lateral- On either side
Contralateral- Opposite sides
Ipsilateral- Same side
The planes of motions to know are the Frontal, Sagittal, and Transverse.
Anatomic Locations
| Plane | Description | Example |
|---|---|---|
| Frontal | Adduction/abduction, Lateral flexion, Eversion/inversion | Lateral raise, lateral lunge, lateral shuffle |
| Sagittal | Flexion and extension | Bicep curl, hamstring curl |
| Transverse | Rotation, Horizontal adduction/abduction | Throwing motion |
Section 9. Joint Motions
Flexion- Muscles shorten
Extension- Muscles lengthen
Plantar flexion- Extension about the ankle joint
Dorsiflexion- Flexion about the ankle joint
Abduction- Extension away from the midline
Adduction- Flexion towards the midline
Horizontal abduction- Abduction along the transverse plane
Internal rotation- Joint rotation towards the midline
External rotation- Joint rotation away from the midline
Section 10. Principles of Human Movement Science
Concentric- Muscle shortens with contraction
Eccentric- Muscle lengthens under resistance
Isometric- Muscle length remains constant against resistance
Length-tension relationship- The tension a muscle can produce at a given resting length
Force-couple- A muscle pair working to produce motion
Force-velocity curve- An increase in velocity correlates to a decrease in concentric force and an increase in eccentric force
Neuromuscular efficiency- The degree at which force can be produced, reduced, and stabilized across all 3 movement planes
Structural efficiency- The degree of optimal alignment of the musculoskeletal system towards the ideal center of mass distribution for a given bodyu
Davis’s law- soft tissue models along the lines of stress
Autogenic inhibition- Muscle spindle inhibition due to sensory impulses of tension being greater than motor impulses of contraction
Reciprocal inhibition- The contraction of one muscle leads to the relaxation of its opposite to facilitate movement
Relative flexibility- The body’s affinity towards seeking the least resistive path
Pattern overload- Abnormal stress caused by excessive repetition of a single movement
Postural distortion patterns- Common movement patterns associated with muscle imbalances
Altered reciprocal inhibition- A tight agonist that inhibits its functional antagonist, causing muscle inhibition
Synergistic dominance- When a synergist takes over a prime mover’s function
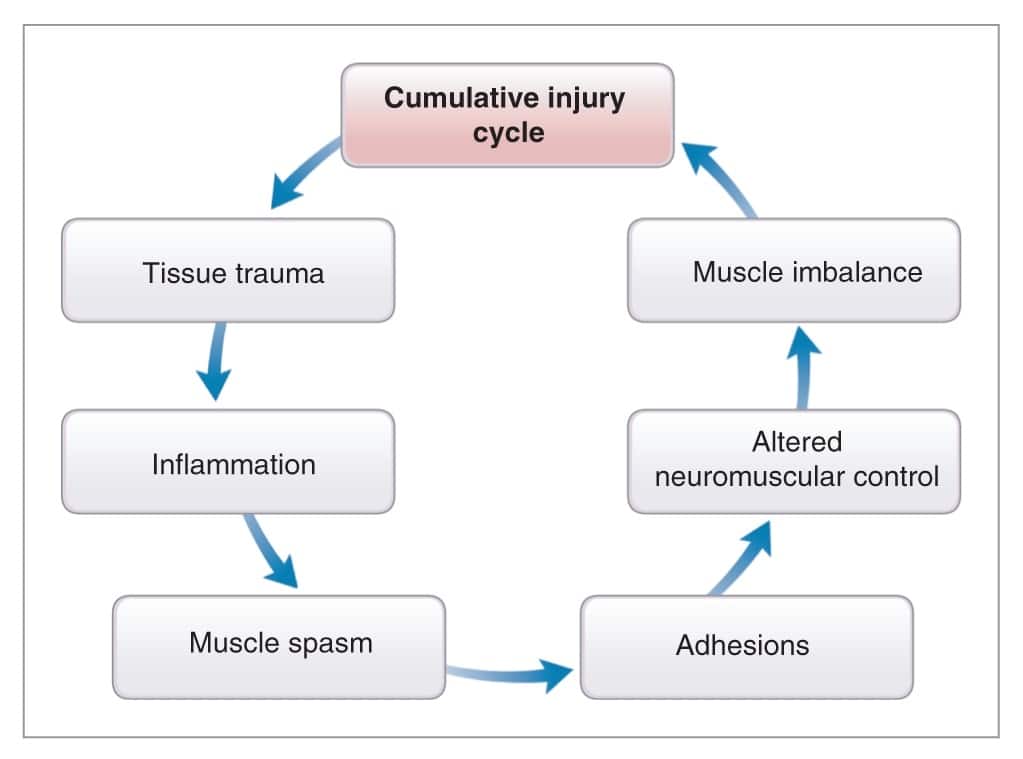
Muscle imbalance- Disproportionate muscle length about a joint
The cumulative injury cycle is essential for the fitness professional to understand that poor posture and repetitive, overuse movements can create dysfunction within the connective tissue of the human body.
The image below is figure 14-12 in the 7th edition.
Section 11. The OPT Model
NASM’s Optimum Performance Training model aimed at enhancing the body through the correction of deficiencies, and improvement of the fundamentals of stabilization, strength, and power
Stability- The ability to achieve and maintain postural equilibrium through all planes of motion
Strength- The degree to which muscular tension can produce force
Strength endurance- The length of time muscular tension can be sustained
Maximal strength- The maximum amount of force that can be produced through muscular contraction
Muscular hypertrophy- The increase in mass and volume of muscle tissue due to growth stimulated by metabolic and/or mechanical response. May lead to a corresponding increase in strength and power.
Power- The rate of strength output over time.
Section 12. Principles of Motor Development
Motor behavior- motor response to internal and external stimuli
Motor control- The integration of present sensory stimuli with previous experiences via the CNS
Motor learning- Incorporation of motor control patterns into adopted movement systems through repetition
Motor development- The lifelong progression of motor skill behavior
Sensorimotor integration- The integration of sensory input with the appropriate motor response
Muscle synergies- Muscles collaboratively recruited by the CNS to produce movement
Proprioception- The ability to interpret sensory input from mechanoreceptors in order to maintain balance and postural equilibrium.
Internal feedback: sensory input data resulting from the corresponding internal response to motor function and its outcomes.
External feedback: explicit data provided by external validators such as a coach, video playback, or readings on measuring implements.
Section 13. Macronutrients
Primary energy source macronutrients that include sugars, starches, and fiber.
Monosaccharide- A single unit of sugar. E.g., fructose, glucose.
Disaccharides- A double sugar molecule. E.g. lactose, sucrose and maltose.
Fiber- Complex polysaccharides found in plant tissue. Assists in gut health, glucose uptake regulation, and the nourishment of gut microbiota.
Soluble Fiber- Soluble fiber dissolves in water.
Insoluble Fiber- Insoluble fiber remains solid/in suspension in water.
Glucose- The most basic molecular structure of a carbohydrate
Glycogen- Carbohydrate storage unit stored in liver and muscle tissue
The Glycemic index refers to numbers (0–100) assigned to a food source that represents the rise in blood sugar after consuming the food.
Lipids are organic compounds made of glycerol and fatty acids that are hydrophobic. They include oils, fats, waxes, and steroids and contain roughly twice the energy yield per unit mass of carbohydrates.
Triglyceride- The most common lipid structure consists of glycerol and 3 fatty acids.
Saturated Fat- A lipid where all the fatty acid chains have single bonds. Solid at ambient temperature.
Trans-fat- Hydrogenated unsaturated fat used for large-scale industrial food production. Known to pose tremendous health risks.
Unsaturated fat- A lipid where one or more double bond in the fatty acid chain.
Monounsaturated- A lipid with only one double bond
Polyunsaturated- A lipid with more than one double bond
Saturated Fat- Meat, dairy products, coconut oil
Monounsaturated fat- tree nuts, flaxseed, sunflower seeds
Polyunsaturated fat- Fatty fish, olive oil
A nitrogen-based organic molecule comprised of one or more amino acid chains.
Sub Molecules of proteins containing amine and carboxyl groups.
Amino acids that are both necessary to normal life function and cannot be naturally produced in the body. They must therefore be ingested through an inclusive diet.
Amino acids that are either unnecessary to normal health, or are necessary, but are naturally produced in adequate quantities and don’t need to be ingested through an inclusive diet.
A protein or protein source that includes all essential amino acids.
A protein or protein source that does not possess all necessary amino acids.
Section 14. Micronutrients
Inorganic molecules that drive important life functions and are only needed in trace quantities. These include vitamins and minerals.
A substance’s ability to have a negative impact on health.
Section 15. Hydration
Approximately 60%.
2.2 L for women and 3 L for men.
Cold water is well known to assist in digestive health.
A beverage containing up to 8% carbohydrates.
Approximately 8oz.
Fatigue decreased performance and circulatory deficiency.
Section 16. Recommendations and Guidelines for Caloric Intake and Expenditure
The amount of heat energy required to raise the temperature of 1 gram of water 1 degree Celsius.
Amount of energy expended during rest and inactivity.
The energy expended through the process of digestion accounts for 6-10% of total expenditure.
Approximately 20% of total energy.
– High carb consumption two to four hours before physical activity
– Consume 1,5 grams of carbs per kg of body weight to maximize glycogen reserves
– For activity lasting more than 1 hour, consume 30 – 60 grams of carbs per hour
Section 17. Dietary Reference Intakes
The guidelines for the ideal intake of a given nutrient.
The mean daily nutritional requirements for an individual of normal health.
The maximum intake level with no perceived health risks.
The ideal recommended nutrient intake for individuals of normal health.
Section 18. Portion Sizes, Meal Timing, and Frequency
The table shows the recommendations for how someone should look to eat when wanting to change their body in the following ways.
Suggested Nutrition For Specific Health Goals
| Weight Loss | Hypertrophy/Lean Mass | General Health |
|---|---|---|
| No more than 10% fat | Eat 4 to 6 meals per day | Incorporate low GI carbs |
| Distribute all macronutrients through the day | Spread protein intake through the day | |
| Consume four to 6 meals per day to control hunger and cravings | Consume carbs and protein within 90 minutes of physical activity for optimal protein synthesis | |
| Avoid calorically-dense processed foods | Maintain healthy ratios of carbs and fats | |
| Hydrate with approx. 9 to 13 cups of water/day | ||
| Measure food portions | ||
| Seek professional supervision for diets under 1200 kcal |
Section 19. Common Nutritional Supplements
Made in the body via the ATP-PC system.
It can boost anaerobic performance and strength output during exercise. It can increase muscle mass over the long term.
Consuming 3-6mg/kg of body weight 1 hour before physical activity has been shown to improve performance.
They are categorically illegal and prohibited by the World Anti-Doping Agency.
Domain 4: Assessment
Section 1. The PAR-Q
1. Determines risk level of exercise for an individual
2. Identifies the need for medical evaluation in an individual
3. Leads to physician referral if the answer is yes to one or more of the questions
Section 2. Elements of Personal, Occupational, and Family Medical History
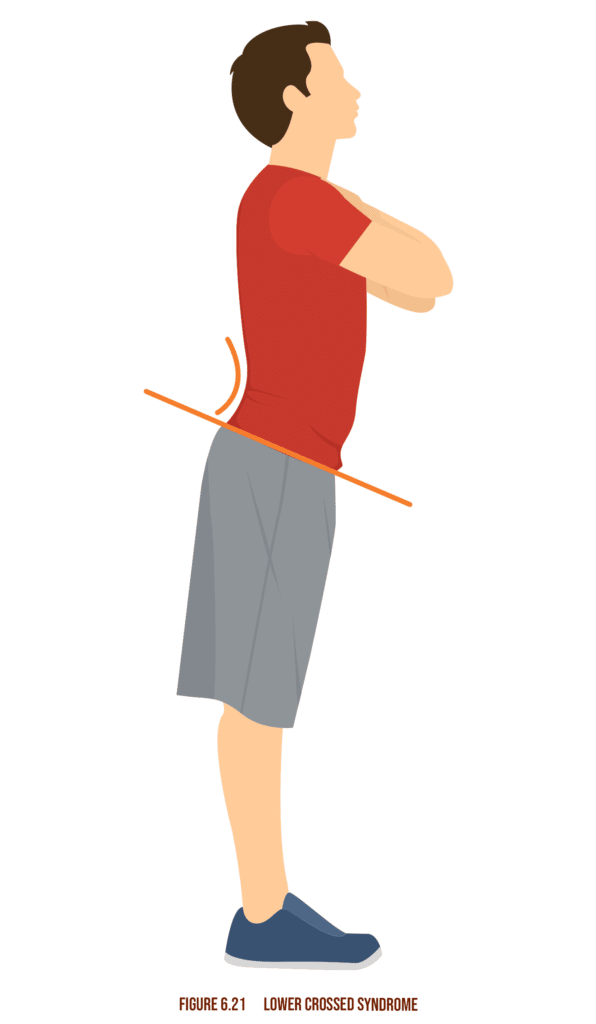
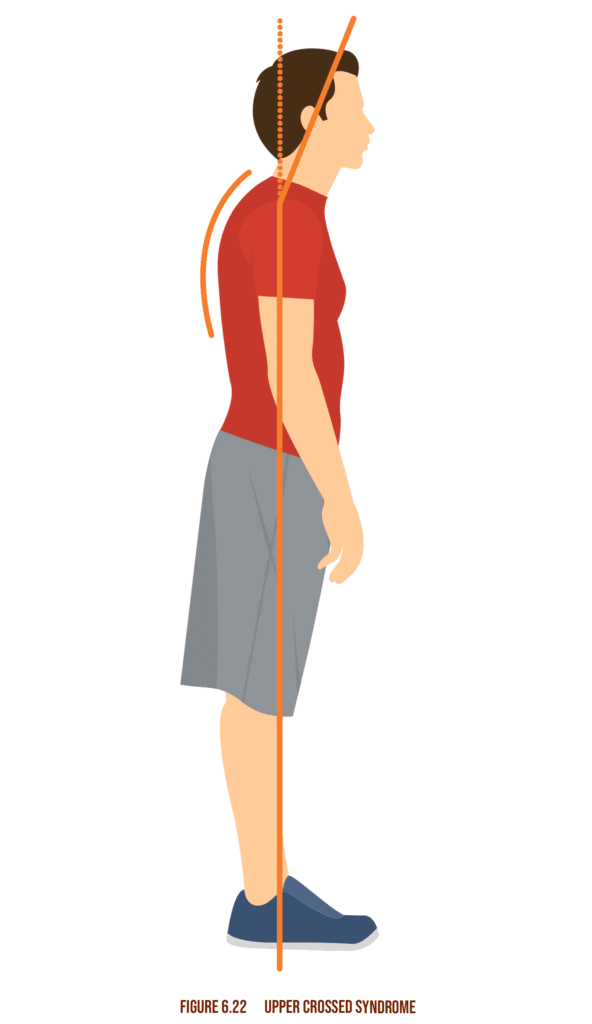
Tightening on the hip flexors, weakening of posterior chain muscles (rounded shoulders and forward head).
Can lead to pattern overload and overuse injuries.
The sustained plantar-flexion can lead to tight calf muscles, leading to over-pronation and weakened dorsiflexion.
– Cardiovascular disease
– Respiratory complications
– Future re-injury
– Neural overcompensation
– Loss of neural control
– Altered neural control
Beta-blockers, heart, and blood pressure medication.
Arthritis, asthma, diabetes, hypertension, obesity, cardiovascular conditions, stroke, cancer, and pregnancy.
Section 3. Cardiorespiratory Assessments
Used to estimate an individual’s VO2max.
The straight percentage method calculated as: HRmax = 220 – age
The regression formula, calculated as: HRmax = 208 – (0.7 × age)
The straight percentage formula is an easier calculation, while the regression formula gives a more accurate reading.
1. Execute 96 steps/minute, on a 12-inch step, over a 3 minute period.
2. Take a 60-second recovery pulse within 5 seconds of stopping
3. Refer to the chart on page 130 of the textbook and match recovery pulse to it
4. Assign the correct heart rate zone: Zone 1: poor – fair
5. Zone 2: average – good
6. Zone 3: very good
1. Document weight
2. 1-mile treadmill walk
3. Document time
4. Record heart rate immediately after
5. Use the VO2 formula to calculate the VO2 score
6. Use the chart on textbook page 132 to match score with age and sex
7. Assign the correct heart rate zones
Zone 1: poor – fair
Zone 2: average – good
Zone 3: very good
Section 4. Physiological Assessments
Place index and middle fingers on the wrist proximal to the thumb.
Less preferred for clients, more suitable for emergency first response, located on the side of the neck.
The heart rate experienced at rest. It can be determined as an average of 3 consecutive morning heart rate readings.
Ave RHR men: 70bpm.
Ave RHR women: 75bpm.
The healthy adult range sits between 70 – 80 bpm.
Systolic: maximum arterial pressure which occurs during cardiac contraction. Health normal of up to 120 mm Hg
Diastolic: minimum arterial pressure which occurs during cardiac relaxation. Healthy normal of up to 90 mm Hg
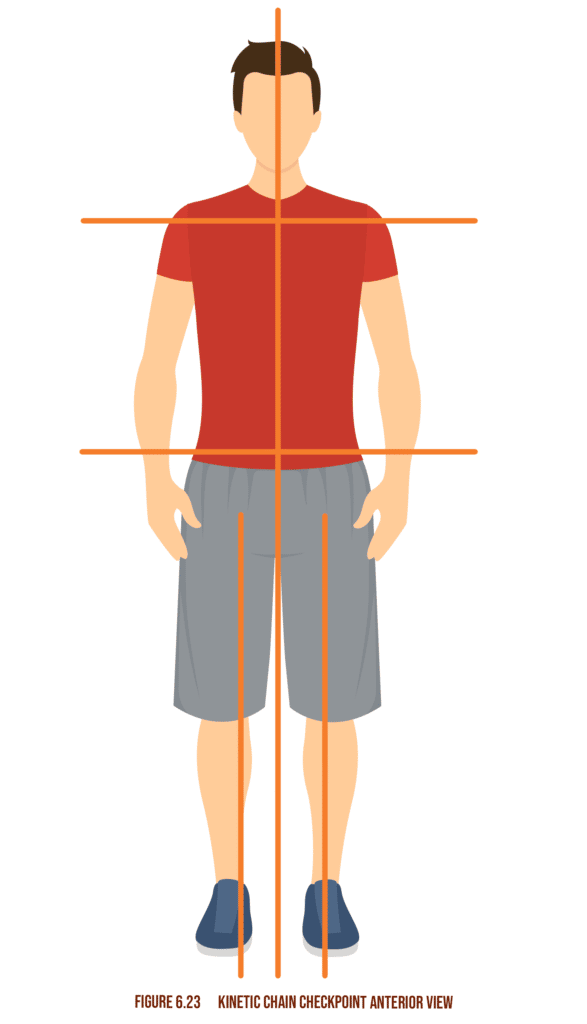
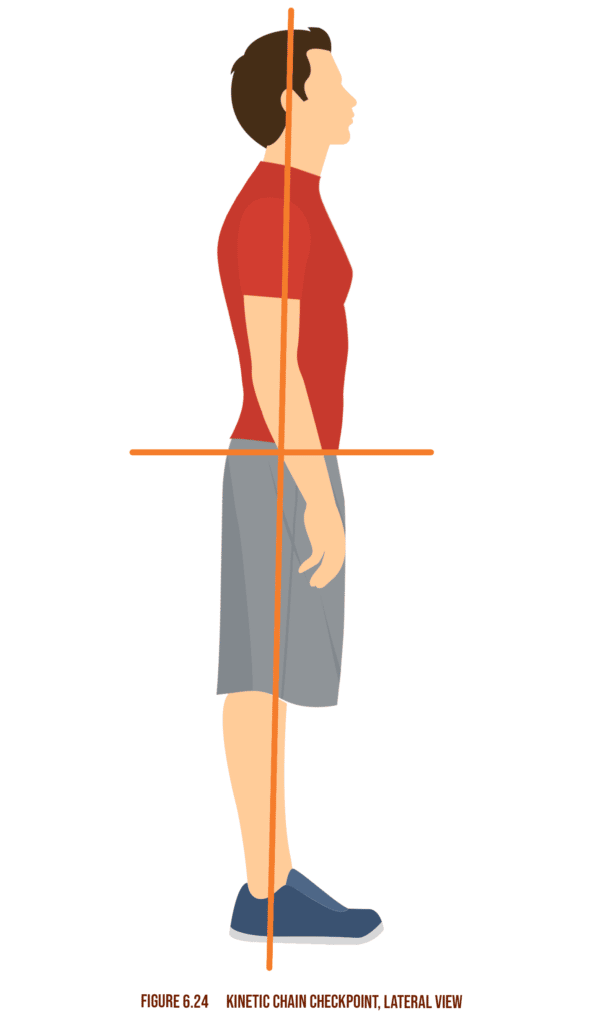
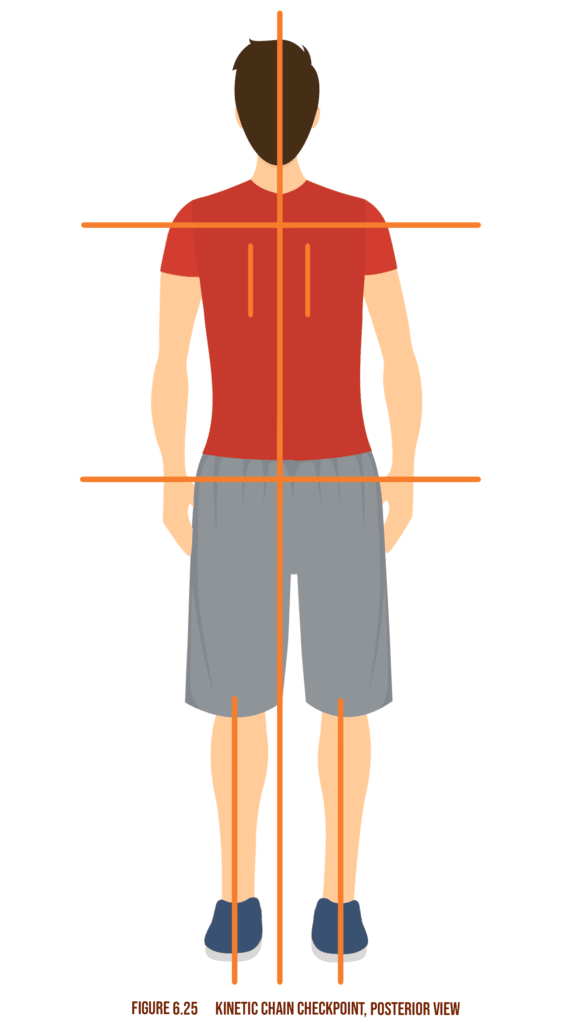
Section 5. Static Postural Assessment
The body’s main joint regions such as knees, elbows, ankles, wrists, head/neck, LPHC, and shoulder girdle.
These static and dynamic postural assessment diagrams are found throughout Lesson 2 of Chapter 12 in the 7th Edition.
Section 6. Assessments from Adjacent Professionals
Cholesterol is a lipid derivative found in the blood and produced in the liver.
HDL is high-density lipoprotein and is a form of cholesterol considered beneficial for health. LDL is low-density lipoprotein and has been linked to an increased risk of cardiovascular disease.
A level of no more than 200 mg/dL.
Section 7. Body Composition Assessments
Any person whose weight sits at no less than 25 lbs above their ideal weight for their height, or anyone with a BMI of 25 to 29.9.
A BMI of at least 30 is classified as obese.
Flexion
Fat mass is calculated as the product of body fat % and total scale weight.
Lean mass is calculated as the total scale weight minus the fat mass.
An electric current is sent through the body and used to determine total fat mass.
Underwater weighing uses the principle that fat mass is more buoyant than lean mass.
Measurements based on changes in girth of several sites such as ankles, chest, waist, hips, calves, and neck. Considered inaccurate.
The waist circumference is divided by the width of the hips. A ratio of no less than 0.8 for females and one of no less than 0.95 for males indicates the potential for obesity-related risk factors.
The weight-to-height ratio of a person. The higher the BMI, the more likely a person is overweight or obese; the lower the BMI, the more likely they are underweight.
Section 8. Performance Assessments
Davies test- An agility and stability test for the upper body
Shark skill test- Neuromuscular control and agility test for the lower body
Bench press test- Determines upper-body maximal strength (1 rep max)
Squat test- Determines lower body maximal strength (1 rep max)
Push-up test- Determines upper body muscular endurance
LEFT test- Determines acceleration, deceleration agility, and neuromuscular control
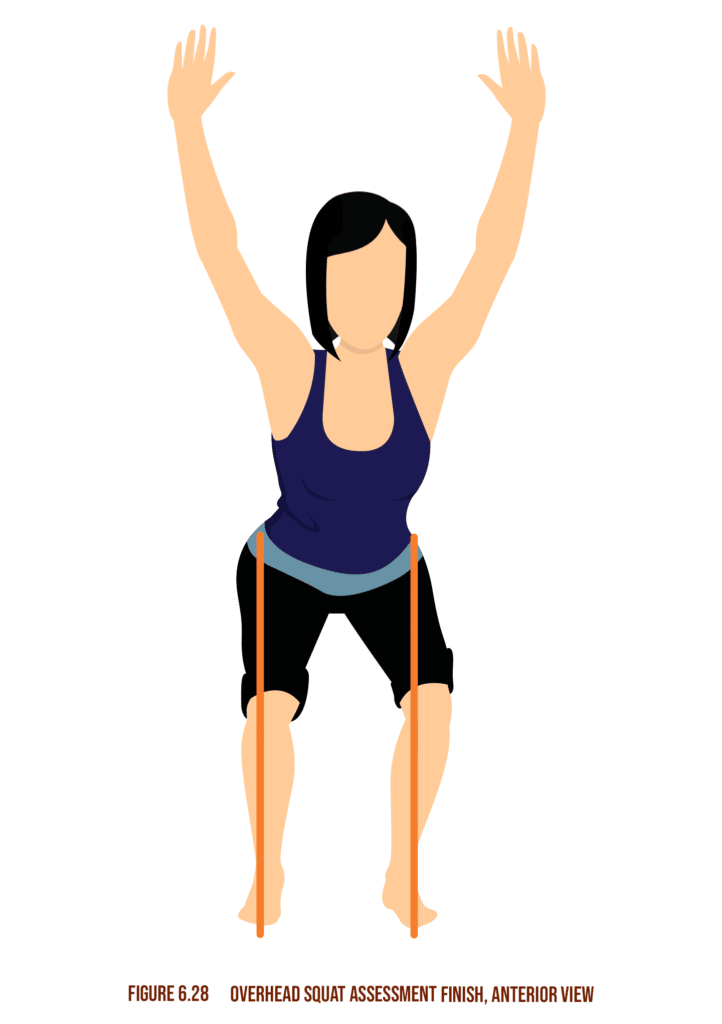
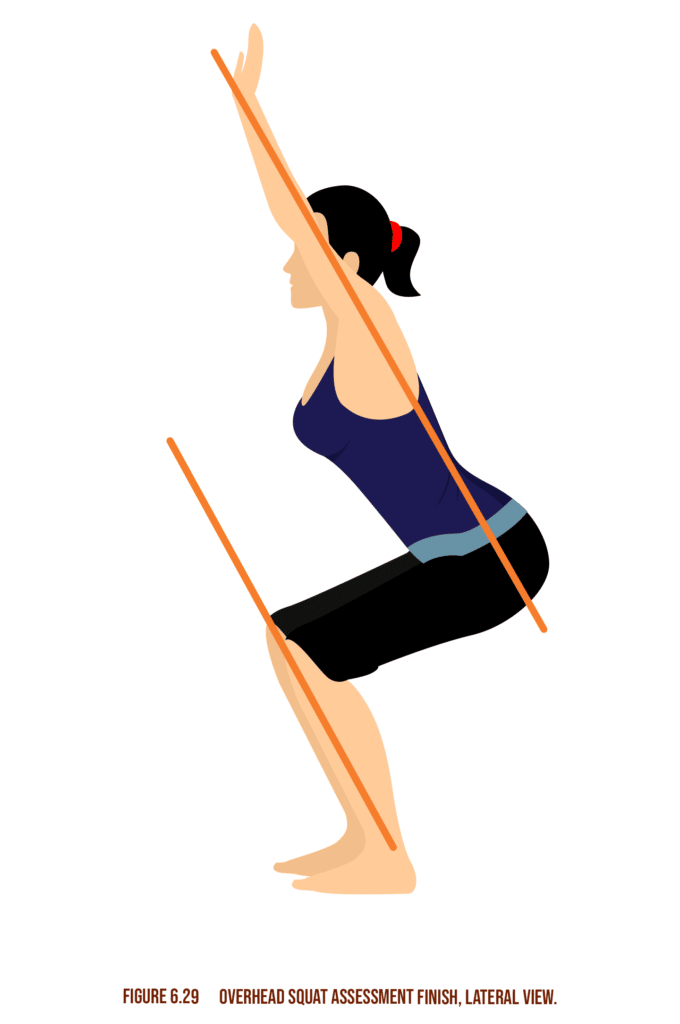
Analyzes posture through movement to determine any movement dysfunctions, imbalances or deviations.
This overhead squat assessment, one of the more important dynamic posture assessments, can be found throughout lesson 3 of Chapter 12 in the 7th Edition.
OHSA Performance Assessment Activity
| View | Kinetic Chain Checkpoint | Compensation | Compensation | Underactive muscles |
|---|---|---|---|---|
| Lateral | LPHC | Pronounced forward lean | Soleus | Anterior tibialis |
| Gastrocnemius | Gluteus maximus | |||
| Hip flexor complex | Erector spinae | |||
| Abdominal complex | ||||
| Anterior pelvic tilt | Hip flexor | Gluteus maximus | ||
| Erector spinae | Hamstring complex | |||
| Latissimus dorsi | Intrinsic core stabilizers | |||
| Posterior pelvic tilt | Hamstring complex | Intrinsic core stabilizers | ||
| Rectus abdominis | Gluteus maximus | |||
| Upper body | Arms shit forwards | Latissimus dorsi | Middle / lower trapezius | |
| Teres major | Rhomboids | |||
| Pectoralis major/minor | Rotator cuff | |||
| Anterior | Feet | Turn out | Soleus | Medial gastrocnemius |
| Lateral gastrocnemius | Medial hamstring complex | |||
| Biceps femoris (short head) | Gracilis | |||
| Sartorius | ||||
| Popliteus | ||||
| Knees | Move inwards | Adductor complex | Gluteus maximus | |
| Soleus | Gluteus medius | |||
| Gastrocnemius | Vastus medialis oblique (VMO) | |||
| Biceps femoris (short head) | ||||
| Tensor fasciae latae (TFL) | ||||
| Vastus lateralis | ||||
| Move outwards | Soleus | Gluteus maximus | ||
| Gastrocnemius | Adductors | |||
| Biceps femoris (short head) | Medial hamstring complex | |||
| Piriformis | ||||
Section 8. Performance Assessments
Assess for the level of ankle proprioception core stability and strength and hip stability and strength.
The Single leg Squat assessment is a slightly more advanced assessment that looks to find problems in dynamic posture. This can be found throughout lesson 3 of chapter 12 in the 7th edition.
Single Leg Squat Performance Assessment Activity
| View | Kinetic Chain Checkpoint | Compensation | Overactive muscles | Underactive muscles |
|---|---|---|---|---|
| Anterior | Knees | Move Inward | Adductor complex | Gluteus medius |
| Biceps femoris | Gluteus maximus | |||
| TFL | Vastus medialis oblique | |||
| Vastus medialis oblique |
Assess for the level of efficiency and identify potential imbalances during pushing movements.
This is another form of dynamic posture assessment that is commonly used. This can be found throughout lesson 3 of chapter 12 in the 7th edition.
Pushing Performance Assessment Activity
| View | Kinetic Chain Checkpoint | Compensation | Overactive muscles | Underactive muscles |
|---|---|---|---|---|
| Lateral | LPHC | Low back arches | Hip flexors | Intrinsic core stabilizers |
| Erector spinae | ||||
| Shoulder complex | Shoulder elevation | Upper trapezius | Mid trapezius | |
| Sternocleidomastoid | Lower trapezius | |||
| Levator scapulae | ||||
| Head | Protrudes | Upper trapezius | Deep cervical flexors |
Assess for the level of efficiency and identifies potential imbalances during pulling movements.
Another form of dynamic posture assessment and this too can be found throughout lesson 3 of chapter 12 in the 7th edition.
Pulling Performance Assessment Activity
| View | Kinetic Chain Checkpoint | Compensation | Overactive muscles | |
|---|---|---|---|---|
| Lateral | LPHC | Lower Back Arches | Hip flexors | |
| Erector spinae | ||||
| Shoulder complex | Shoulder elevation | Upper trapezius | Mid trapezius | |
| Sternocleidomastoid | Lower trapezius | |||
| Levator scapulae | ||||
| Head | Protrudes | Upper trapezius | Deep cervical Sternocleidomastoid flexors |
Assess for level of efficiency and identify potential imbalances during walking and running.
The gait cycle is discussed throughout lesson 1 of chapter 19 in the 7th edition.
Gait Performance Assessment Activity
| View/Checkpoint | Compensation | Overactive muscles | Underactive Muscles |
|---|---|---|---|
| Feet | Flatten | Peroneal complex | Anterior tibialis |
| Lateral gastrocnemius | Posterior tibialis | ||
| Biceps femoris (short head) | Medial gastrocnemius | ||
| TFL | Gluteus medius | ||
| Turn out | Soleus | Medial gastrocnemius | |
| Lateral gastrocnemius | Medial hamstring | ||
| Biceps femoris (short head) | Gluteus medius/maximus | ||
| TFL | Gracilis | ||
| Sartorius | |||
| Popliteus | |||
| Knees | Move inward | Adductor complex | Medial hamstring |
| Biceps femoris (short head) | Medial gastrocnemius | ||
| TFL | Gluteus medius/maximus | ||
| Lateral gastrocnemius | Vastus medialis oblique | ||
| Vastus lateralis | Anterior tibialis | ||
| Posterior tibialis | |||
| LPHC | Low back arch | Hip flexor complex | Gluteus maximus |
| Erector spinae | Intrinsic core stabilizers | ||
| Latissimus dorsi | Hamstrings | ||
| External obliques | Sartorius | ||
| Adductor complex | Popliteus | ||
| Excessive rotation | Hamstrings | Gluteus medius/maximus | |
| Intrinsic core stabilizers | |||
| Hip hike | Quadratus lumborum (opposite side) | Adductor complex (same side) | |
| TFL/gluteus minimus (same side) | Gluteus medius (same side) | ||
| Shoulders | Rounded | Pectorals | Middle and lower trapezius |
| Latissimus dorsi | Rotator cuff | ||
| Head | Forward | Upper trapezius | Deep cervical flexors |
| Levator scapulae | |||
| Sternocleidomastoid |
Section 10. Performing Assessments with Special Populations
A modification of the single-leg squat assessment to a single-leg balance assessment as well as a reduction in ROM of the overhead squat. Push up an assessment to pivot off the knees instead of the feet. Avoid power and impact-based exercises and assessments.
For cardio assessment, the Rockport walk test is the ideal assessment. Institute a single-leg balance test instead of the single-leg squat and implement the push-up test with the knees as the pivot and an elevation for the hands, such as a bench.
Section 11. Indicators that a Client’s Condition is Outside Scope of Practice
Medical diagnosis- Prescription of pharmaceuticals and treatment of any medical condition
Diet prescription and therapy- Psychoanalysis, psychotherapy, or mental health counseling
Section 12. Criteria For Reassessment
-After a four-week period where changes in programming are occurring
-After notable indications of improvement
-When new goals have been identified and selected by the client
-When notable changes in lifestyle behaviors occur, such as dietary, career, relinquishing of previous addictions, etc…
Corrective flexibility should be implemented in phase 1 of training and helps increase ROM, addresses imbalances, and correct deviated movement patterns.
Best implemented at phases 2, 3, and 4. It helps promote improved neuromuscular efficiency, soft tissue extensibility, and reciprocal inhibition.
Best implemented at phase 5 of training. This type of flexibility promotes and maintains integrated, multiplanar soft tissue extensibility while optimizing neuromuscular control.
Gentle massaging motions using a rigid, smooth implement such as a foam roller to ease and release knots in the muscle tissue. This relieves tension and autogenic inhibition.
Stretching muscle just past the comfortable tension limit and holding the extension for at least 30 seconds.
Dynamic movement of joints into a ROM by agonists and synergists.
It uses the production of force to move joints through a full ROM.
Domain 5: Exercise Technique and Training Instruction
Section 1. Exercise Set-up and Technique
– Asses set-up and correct technique of all documented exercises-
– Categorize all exercises
– Regress each exercise
– Progress each exercise
– Perform each exercise
– Boost respiratory and heart rate
– Boosts cardiac output for exercise
– Boosts circulation to active muscles
– Boost oxygen uptake and use capacity
– Boosts temperature of active tissues
– Boosts rate of muscular contraction
– Boosts metabolic activity
– Boosts extensibility of soft tissue
– Boost mental focus and readiness for exercise
Low-intensity movement unrelated to specific training activities would fall under general warm-up, while a specific warm-up would entail low-intensity movements that directly mimic the intended training activity.
Gradual 5-10 minute transition from active to steady-state utilizing light cardio, static stretching, and SMR.
Concurrent extension or flexion of hip, knee, and ankle.
Section 2. Kinesthetic, Auditory, and Visual Cueing
The information produced by sensory input and sensorimotor integration leads to permanent pattern development.
External feedback is provided explicitly by external mediators while internal feedback is tacit recognition of intrinsic effects/changes.
Audiovisual through an instructor or playback system and knowledge of results.
– Tell (auditory cueing)
– Show (visual cueing)
– Direct (kinesthetic cueing)
Section 3. Safe Training Practices
What:
Is safe?
Is a contraindication?
Is an Appropriate Intensity?
How:
How many exercises?
Sets and Reps?
Days per week?
Section 4. Safe and Effective Spotting Techniques
– Determine total reps to be performed
– Only take weight where there is immediate danger of dropping
– Only assist just enough to overcome the ”sticking point”
– Spot wrists and not elbows during dumbbell workouts
– Avoid spotting machine-based exercises by positioning your hands under the weight stack.
Section 5. Proper Breathing Technique
– Shallow breathing may be due to the use of secondary respiratory muscles instead of the diaphragm
– Respiratory muscle overactivity may result in headaches and dizziness
– Excessive breathing can lead to oxygen/CO2 imbalance and retention of waste molecules.
Instruct breathing through the stomach in order to normalize.
Domain 6: Program Design
Section 1. Resistance Training Systems
Training one set per exercise. This is an ideal protocol for beginners.
Multiple sets per exercise.
Training where the intensity increases or decreases progressively with each set.
Performing two consecutive sets of exercises with very little to no rest in-between.
Performing multiple exercises with little rest between sets.
A circuit training variation that alternates upper and lower body training for optimized circulation.
Compartmentalizing training focus between the upper and lower body and dedicating entire sessions accordingly.
Alternating training focus between the upper and lower body with each set.
Focusing on all exercises for one body segment and then moving on to the next within one session.
Section 2. Resistance Training Methods
This information is taken from chapter 21 of the 7th edition.
Resistance Training Methods
| Stabilization | Strength | Power |
|---|---|---|
| Method | ||
| 4/2/1 tempo, lower weight, and higher reps in an unstable, but controlled, environment | 2/0/2 tempo, moderate to heavyweight, low to moderate reps with full ROM | Explosive tempo, light weight, moderate reps with full ROM |
| Exercises | ||
| Ball squat, curl to press | Lunge to two-arm dumbbell press | Two-arm medicine ball chest pass |
| Multiplanar step-up balance, curl, to overhead press | Squat to two-arm press | Rotation chest pass |
| Ball dumbbell chest press | Two-arm push press | Ball medicine ball pullover throw |
| Barbell clean | Barbell clean | Wood chop throw |
| Standing cable row | Flat dumbbell chest press | Medicine ball scoop toss(shoulders) |
| Ball dumbbell row | Barbell bench press | Medicine ball side oblique throw |
| Single-leg dumbbell scaption | Seated cable row | Squat jump |
| Seated stability ball military press | Seated lat pull | Tuck jump |
| Single-leg dumbbell curl | Seated dumbbell shoulder press | |
| Single-leg barbell curl | Seated shoulder press machine | |
| Supine ball dumbbell triceps extension | Seated two-arm dumbbell biceps curls | |
| Prone ball dumbbell triceps extension | Biceps curl machine | |
| Biceps curl machine | Cable pushdowns | |
| Multi-planar step-up to balance | Supine bench barbell triceps extension | |
| Leg press | ||
| Barbell squat |
Section 3. Cardiorespiratory Training Methods
Cardio training was instituted progressively to avoid injury and over-training.
Characterized by initial cardio activation for sedentary individuals. Implemented at HR zone 1. Starts slow and progresses up to about 30-60 mins of training.
Characterized by cardio progress for intermediate-level individuals. Implemented at HR zone 2 intervals, with HR zone 1 for recovery. 1 min zone 2:3 min zone 1 (1:3 work/rest ratio).
Characterized by cardio progress for advanced-level individuals. Implemented at HR zone 3 intervals, with HR zone 2 for recovery and HR zone 1 as a warm-up. 1 min zone 3:1 min zone 2 (1:1 work/rest ratio).
Section 4. Core Training Methods
For effective global stability of all movement chains through the body. Develops local stabilization muscles, muscle balance, and correct transfer of force.
Core stabilizer recruitment is activated by pulling the navel towards the spine (local stabilization).
Stabilizing the LHPC through contraction of the anterior and posterior core muscles as well as the glutes (global stabilization).u003cbru003e
Section 5. Balance Training Methods
– Develops awareness of balance limit/threshold
– Optimizes synchronicity and synergy of muscle firing patterns, in turn improving joint stability.
– Combines functional training with proprioceptive activation.
– Maximizes sensory input to CNS, in turn, maximizes the efficiency of relevant motor response.
Section 6. Proprioceptive Manipulation
– Stable to unstable
– Static to dynamic
– Slow to fast
– Two limbs to single limbs
– Open eyes to closed eyes
– Known to unknown
– Supine
– Prone
– Lateral lying
– Kneeling
– Half- kneeling
– Standing
– Two legs
– Single leg
– Two leg (unstable)
– Single leg (unstable)
– Solid floor
– Balance beam
– Half-foam roll
– Foam pad
– Balance disk
– Wobble disk
Section 7. Plyometric Training Methods
Power-focused movement training consisting of an eccentric phase for potential energy development followed by an explosive concentric phase.
Transitional phase between eccentric and concentric action during a plyometric movement. The shorter the transition phase, the more powerful the movement.u003cbru003e
Section 8. SAQ Training Methods
Speed, Agility, and Quickness. Relates dynamic reactivity and the ability to accelerate, decelerate and change position and direction in all planes of motion while maintaining dynamic stability.u003cbru003e
Cone and agility ladder drills.
Section 9. Exercise Progression/Regression
Allows for managed progress and development of skills.
Section 10. General Adaptation Syndrome
The body’s 3 stage response to stress. The stages are alarm, resistance development, and exhaustion.
The primary response to a stressor leads to the engagement of protective systems.
Functional adaptation to the stressor leading to tolerance of that current level of stress.
Sustained stress over an excessive period or intensity leads to system failure and break down of adaptation.
Section 11. Principle of Specificity
Stands for Specific Adaptation to Imposed Demands. This refers to the fact that exposing the body to specific stressors through training will lead to an adaptation that matches those specific demands.
The specific forces and direction through which they are applied.
The sensory inputs and the corresponding motor responses.
The energy demands and biochemical activity are relevant to the specific demands.
Section 12. Principle of Overload
Training stimuli and demands must be progressively elevated through an increase in intensity and/or volume in order to promote sustained optimization of adaptation.
Section 13. Principle of Variation
The principle works by reducing risk of exhaustion while maintaining ideal overload and maximizing kinetic chain stimulation.
Section 14. Periodization Concepts
Dividing training into specific periods called cycles is designed to optimize adaptation both over long-term and short-term periods.
A training plan is split into weekly, monthly, and annual cycles that progress from high-volume, low-intensity workouts to low-volume, high-intensity workouts.
Progressively changing the OPT phases as the program runs while still adhering to recovery protocols.
Section 15. Acute Variables
Level of effort or resistive force required to perform an exercise.
Quantity of complete efforts or repetitions in given time required to complete an exercise set or workout session.
The FITTE principles are found throughout chapter 15, lesson 6 in the 7th edition. Ans this also adds in volume and progression, which are less talked about.
FITTE Principles Chart
| Column 1 | Column 2 | Column 3 |
|---|---|---|
| F | Frequency | Total number of training sessions per unit time |
| I | Intensity | Level of effort required to successfully perform exercises |
| T | Time | The period in which training occurs |
| T | Type | The nature of physical activity engaged |
| E | Enjoyment | The amount of pleasure derived from performing the exercise or workout |
– hypertrophy
– healthy cholesterol balance
– improved metabolism
The principle works by reducing the risk of exhaustion while maintaining ideal overload and maximizing kinetic chain stimulation.
Section 16. Modality Risks and Rewards
Training using one’s own physical mass as a training load through all planes of motion.
Using ropes and webbing to create a proprioceptively rich training environment.
Movement of external load through multiple planes of motion while anchoring to a stable base. E.g. dumbbells, barbells, kettle-bells, medicine balls and sandbags.
Ideal for beginners with limited stability adaptation and ROM.
Proprioceptive modalities are used to create instability during exercise, thus leading to a proprioceptively rich training environment that causes adaptations towards balance and stability. Equipment includes an unstable surface of the apparatus.
Section 17. Overtraining, Rest, and Recovery
– Fatigue
– Performance decline
– Irregular sleep patterns
– Reproductive health issues
– Compromised immunity
– Unstable mood
– Appetite decrease
– Hormonal imbalance
Section 18. Current Trends and Their Application to Training
– Provides constant, sustained guidance and feedback
– Can manage and assess all variables
– Allows for remote client management
– Optimized nutritional management
1. Provides exercise data and feedback
2. Monitors vitals and sleep habits
3. Provides information on progress and incentivizes it
1. Powerful marketing tool for services
2. PR and reputation management
3. Provide value through information and useful content
4. Inspire clients and prospects
5. Network with peers and collaborators. Study and learn from competitors
Wearable fitness trackers.
Section 19. Program Design for Special Populations
This is a focus of lesson 1 in chapter 23 of the 7th edition.
Youth Training Considerations
| Column 1 | Column 2 |
|---|---|
| Mode | Moderate cardio (jogging, walking, running), sports, and games. Resistance training |
| Intensity | Moderate to vigorous |
| Frequency | 5 to 7 days per week (cardio) |
| Duration | No more than 1 hour per day |
| Flexibility | Adhere to OPT flexibility protocols |
| Resistance Training | Frequency: 2-3 days/ weekSets: 1-5 setsRepetitions: 3-30/setIntensity: 45%-85% of 1-RM |
| Special Considerations | Activity should be enjoyable and based on the quality of postural control and less on the intensity |
This table also comes from lesson 1 of chapter 23 in the 7th edition.
Older Adult Training Considerations
| Column 1 | Column 2 |
|---|---|
| Mode | Stationary cycling, treadmill with handrail, aquatic aerobics |
| Intensity | 40-85% of VO2max |
| Frequency | 3-5 days/week moderate, 3 days/week vigorous |
| Duration | 30-60 mins/day. 8-10 min bursts |
| Flexibility | SMR and static stretching exercises |
| Resistance Training | Frequency: 3-5 days/ weekSets: 1-3 setsRepetitions: 8-20/setIntensity: 40-80% 1-RM |
| Special Considerations | Slow and well-monitored progress. Progress exercises toward free sitting or standing. Regular breathing avoiding Valsalva maneuver Implement slow, active, or dynamic stretching in case SMR or static stretching is poorly received. |
This is featured in lesson 6 of chapter 23 in the 7th edition.
Pregnancy Training Considerations
| Column 1 | Column 2 |
|---|---|
| Mode | Low impact cardio (treadmill, stationary bike) no sudden or jarring motions |
| Intensity | Stage 1 cardio. Stage 2 if medically cleared |
| Frequency | 3-5 days/week cardio |
| Duration | 15-30 mins/day |
| Flexibility | SMR, static and active-isolated stretching |
| Resistance Training | Frequency: 2-3 days per week Sets: follow OPT Phase Repetitions: 12-15 per set intensity: light loads Only OPT Phases 1 and 2 are advised; use the only Phase 1 after the first trimester. |
| Special Considerations | No prone or supine exercises beyond the 12th week of pregnancy. No SMR on varicose vein regions and swollen areas. No plyometric exercises during the second and third trimesters. No power or speed assessment. Pivot push-up assessment from knees instead of feet. Change the single-leg squat to a single-leg balance assessment. Reduce ROM for the overhead squat assessment. |
This is featured in lesson 2 of chapter 23 of the 7th edition.
Obesity Training Considerations
| Column 1 | Column 2 |
|---|---|
| Mode | Low impact cardio (treadmill, stationary bike) no sudden or jarring motions |
| Intensity | 60-80% HR max.; can be adjusted to 40-70%; use the talk test |
| Frequency | 5-7 days/week cardio |
| Duration | 40 - 60 mins/day. 2x 20-30min/day |
| Flexibility | Stretches performed seated or standing, use SMR if possible |
| Resistance Training | Frequency: 2-3 days/week. Sets: 1-3 sets. Repetitions: 10-15 /set. Intensity: follow OPT Phases Implement circuit training for Phases 1 and 2 |
| Special Considerations | Exercise should be performed standing or seated when possible. Watch for other obesity-related chronic diseases. Use the Rockport walk test for cardiac assessment. Pivot push-up assessment from knees instead of feet. Test single-leg balance instead of single-leg squat assessment. |
This is featured in lesson 4 of chapter 23 in the 7th edition.
Hypertension Training Considerations
| Column 1 | Column 2 |
|---|---|
| Mode | Stationary cycling, treadmill walking, rowers |
| Intensity | 50-85% HR max., can adjust to 40-70%. Stage 1 cardio progressing to stage 2 cardio |
| Frequency | 3-7 days/ week cardio |
| Duration | 30-60 minutes/day |
| Flexibility | Static and active-isolated stretching; standing or seated |
| Resistance Training | Frequency: 2-3 days/week Sets: 1-3 sets Repetitions: 10-20/set Intensity: Adhered to OPT Phase protocols, no more than 1 second for isometric and concentric muscle activity. Implement circuit or PHA training systems with adequate recovery. |
| Special Considerations | No heavy lifting or Valsalva maneuver. Avoid over-gripping weights or clenching fists during workouts. Perform exercises in a standing or seated position. Stand up slowly to avoid vertigo/dizziness. Slow progression |
This is featured in lesson 5 of chapter 23 in the 7th edition.
Osteoporosis Training Considerations
| Column 1 | Column 2 |
|---|---|
| Mode | Treadmill with handrail |
| Intensity | 50-90% HR max. Stage 1 cardio progressing to stage 2 |
| Frequency | 2-5 days/week cardio |
| Duration | 20-60 min/day. 8 -10min bouts |
| Flexibility | Static and active-isolated stretching |
| Resistance Training | Frequency: 2-3 days/week Sets: 1-3 sets Repetitions: 8-20/set Intensity: max of 85% 1-RM |
| Special Considerations | Slow progress Progress to free sitting/standing if possible Hips, thighs, back, and arms focal areas Avoid excess loads on the spine Avoid the Valsalva maneuver. |
NASM Study Guide Overview
Seeking the all-around greatest, free NASM Study Guide?
Worry not; we’ve got you covered!
With this carefully crafted NASM CPT exam study guide, you increase the chances of passing your NASM certified personal trainer exam!
Upon finishing the NASM certification study guide, you will cover the following, so make sure to bookmark this page.
- Specific questions, figures, and charts that apply to exam questions
- Insight into the NASM CPT test
- Proven study methods from NASM-CPTs
This guide is meant to cover all the bases you need to know for the biggest personal trainer certification of them all: the NASM CPT certification.
The National Academy of Sports Medicine’s trainer program is also one of the harder certs to pass on a first attempt (unlike the ISSA CPT which the easiest exam) so you want to make sure you understand what will be tested on from top to bottom!
This CPT study guide has been shown to work for the majority of users, and we enjoy hearing from these users and their success on the NASM exam. Be sure to combine them with practice tests as part of your NASM education to ensure you know the material.
Combined with resources like the NASM book, answer explanations, and breakdown of all the subjects and domains that students need an understanding of, you can certainly join the thousands of individuals who have earned their NASM certification card.
NASM is among the hardest personal trainer exams, standing out from organizations like ACE and others due to the complexity of the items. Be sure to take notes to ensure the accuracy of each question you answer.
Before you know it, you’ll be the most qualified trainer in the gym with a passion for excellence and a job guarantee that’s sure to keep you employed. Are you ready to be a formidable force ready to help everyone reach their fitness goals from gyms to studios?
We hope you’ve enjoyed using the best study guide for NASM. It was crafted and put together by qualified trainers who have been through the works and passed the NASM CPT exam.
FAQs
How long does it take to study for the NASM exam?
Generally, this will be around 3 – 6 months for people who have little experience with exercise science. For People with more experience going in, this could be lessened.
What does a NASM study schedule look like for someone wanting to pass the exam?
We recommend 1 chapter per week to help with retaining the information. This is the most successful schedule for ensuring you understand the information well.
What is the NASM study guide?
This is NASM’s most expensive version of their study guide for exam prep, and something we look to emulate with our study guides offered on this website.
What is the difference between the 6th and the 7th Edition NASM CPT study guides?
The 7th Edition is updated to suit the new domain format and make the information easier to study. Both versions can be used for the current exam, but the 7th edition is newer and more optimized for studying.
Can you just study the study guide NASM CPT?
While it is recommended to not only study for your NASM CPT with the textbooks and study materials, you may study the NASM CPT study guide as well, or by itself. This really depends on what kind of learner and test taker you are.
Do I need to study the NASM study guide?
Now, it’s important to know that nobody but you can make choices for yourself! It is wise to study the NASM study guide. The NASM study guide covers everything you’ll need to know for your NASM exam.
Is the NASM study guide enough for the exam?
This comprehensive NASM self-study guide will definitely succeed in helping you pass your CPT exam! However, note that it is still recommended to review the other NASM study materials as well.
What are the prerequisites for enrolling in the NASM CPT study program?
In order to be eligible to become a NASM-CPT, you must be 18 years of age, have a current and valid high school diploma GED or the equivalent, and have proof of both CPR and AED certification.
Is the NASM study guide accurate?
Yes. The NASM exam study guide is very accurate and covers all things training!
Besides this guide, we have a number of other awesome NASM study materials that will help you gain that edge when it’s time to take the test. Our paid study guide for NASM CPT covers more depth.
This is what makes it the best NASM personal trainer study guide!
Be sure to check out the rest of Trainer Academy’s NASM study options as well as a whole host of guides and materials for other popular certifications such as.
- ACE CPT MVP Study Package
- NSCA CSCS MVP Study Package
- ISSA MVP Study Package
- NSCA CPT MVP Study Package
- ACSM MVP Study Package
Additional NASM Study Tips
Don’t forget to download our 14 step NASM CPT exam preparation checklist to ensure that you pass the test.
- Study frequently and on a schedule.
- Make mnemonics to help with memorization of difficult topics.
- Print the diagrams, figures, and charts.
- Go through the study materials and practice test questions.
- Breeze through the NASM Essentials of Personal Fitness Training text on your own.
- Create flashcards and answers for the NASM study guide.
Good luck with your NASM-CPT exam!
References
- Adams A. Periodization Training Simplified: A Strategic Guide | NASM Blog. blog.nasm.org. Published 2022. https://blog.nasm.org/periodization-training-simplified
- Kharb P. The Learning Styles and the Preferred Teaching–Learning Strategies of First Year Medical Students. JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH. 2013;7(6). doi: https://doi.org/10.7860/jcdr/2013/5809.3090
- Koohestani HR, Baghcheghi N. A comparison of learning styles of undergraduate health-care professional students at the beginning, middle, and end of the educational course over a 4-year study period (2015–2018). Journal of Education and Health Promotion. 2020;9(208). doi: https://doi.org/10.4103/jehp.jehp_224_20









